Soft sonor [L'] appears in a child’s speech in the second or third year of life, hard [L] - at 5-6 years, which is associated with more complex articulation, requiring strong muscles of the tip of the tongue and its upper rise. In the absence or distorted pronunciation of a phoneme, lambdacism is diagnosed; when it is replaced with other speech sounds, paralambdacism is diagnosed. Along with sigmatisms and rhotacisms, pronunciation defects [L-L'] are among the most common sound distortions among preschool children with speech disorders (from 10% with dyslalia to 46.7% with erased dysarthria).
Causes of lambdacism
Deficiencies in pronunciation [L-L'] are typical for children suffering from functional and mechanical dyslalia, dysarthric disorders, and open rhinolalia. Organic defects in the peripheral speech organs, impaired muscle innervation, and functional insufficiency of sound pronunciation can lead to lambdacism:
- Shortened hypoglossal ligament.
It does not allow the upward movement of the tongue, which is necessary for the formation of the desired articulatory pattern. As a result, the child finds an available compensatory position (interdental, labiodental, etc.), which replaces correct articulation. - Macroglossia and microglossia.
If the language is underdeveloped, it becomes impossible or difficult to pronounce all linguistic phonemes, including dental [L-L']. The small size of the organ makes it impossible for the tongue to approach the upper incisors. With a massive tongue, both its upper rise and narrowing of the tip are difficult. - Changes in muscle tone.
With dysarthria, the tongue may be flaccid, paretic or tense and spastic. These factors significantly distort articulation. The tone of the orbicularis oris muscle is also impaired, which is accompanied by difficulties in voluntarily opening and holding the lips. - Palatal clefts.
Compensatory features for rhinolalia are a high elevation of the root of the tongue, a shift of articulation into the depths of the oral cavity, and non-participation of the tip of the tongue in the formation of sounds. [L] is usually absent or appears bilabial. - Hearing loss.
Hearing loss can be accompanied by both mixing and substitution of sound due to impaired acoustic differentiation, and distorted pronunciation due to inaccuracy and blurred articulation. - Other reasons.
Lambdacism can be caused by the lack of formation of correct speech kinesthesia as a result of speech deprivation and sickness in children. Another reason is copying incorrect sound pronunciation, including dialectal features in a bilingual environment.
Topic 8. Lambdacism and its correction
Disadvantages of pronunciation of sounds l
and
l'
are called lambdacism. Those varieties of the defect that are expressed in the replacement of these sounds with some others are called paralambdacism.
Articulation of the sound l
is as follows. The position of the lips depends on the subsequent vowel pronounced. The upper and lower incisors are located at a slight distance from each other. The tongue rests its tip on the upper incisors or their gums. The lateral edges of the tongue do not meet the molars, leaving passages for exhaled air on the sides. The root part of the tongue is raised, due to which, in the presence of lateral passages on both sides, the tongue takes the shape of a saddle. The soft palate is raised, covering the passage to the nose. The vocal folds are closed and vibrate.
Soft sound l (l')
differs in articulation from the hard one in that it is not the root part of the tongue that rises, but the anterior-middle part of its back;
Not only the tip of the tongue meets the gums, but also a significant surface of the front part of the back with the alveoli. Often l'
is generally pronounced with the tip of the tongue lowered by closing the front part of the back with the alveoli (Fig. 7).
Violation of both hard and soft tissues
is very rare. Usually only the hard sound is pronounced incorrectly. This is explained by the fact that it is more complex in articulation.
Disadvantages of pronunciation of the phoneme l
have a number of varieties.
This includes: lengthening adjacent vowels (“aampa”, “paaka”, “stoo” instead of lamp, stick, table);
pronouncing
l
in the form of a short vowel sound like
y
(“yampa”, “payka”, “stoy”);
replacing l with
the phoneme
й (j)
(“yampa”, “soldering”, “stop”), the phoneme
l’
(“lamp”, “palka”, “so”), the phoneme
n
(“nampa”, “punka”, “ moan");
pronouncing l in
the form of a back-lingual nasal sound ng
“ngampa”, “ngapa” instead of lamp
The most common type of lambdacism is pronounced as l
sound
in
or short
y.
At the same time, the tongue is pulled back into the mouth, as with the vowel
y.
Among the anomalies in the anatomical structure of the speech apparatus that predispose to lambdacism, one should name a short hyoid frenulum.
The following techniques are used to correct lambdacism. First, the child is given a task according to the proposed model, using a mirror, freely stick out his tongue and hold it between his teeth. Then he must, without changing the position of his tongue, pronounce a
or
s.
Now the speech therapist only formulates the instructions, and he himself articulates in front of the mirror without a voice.
Already with this position of the speech organs, a drawn-out l can be obtained,
which, however, should not be drawn to the child’s attention, so that he does not stray into his usual pronunciation.
The first exercises aimed at consolidating the resulting articulation come down to pronouncing the resulting sound in syllables with a vowel a
: first in a closed syllable
(al),
then between vowels
(ala)
and finally in an open syllable
(la).
Next, syllables with vowels
ы, о, у (ala, aly, alo, alu, la, ly, lu,
etc.) are introduced.
In cases where lambdacism affects not only l, but also its soft pair - l'
, correction of the first sound serves as a reliable basis for mastering the second.
The latter is usually easily achieved in open syllables with front vowels (li, le),
and then with other vowels when comparing syllables including l
and
l
(la-la, lo-le, lu-lyu).
Once the correct articulation of the sound l
and exercises have been done to consolidate it on the material of syllables, words and phrases; in cases of paralambdacity, it is necessary to carry out a series of exercises aimed at developing the differentiation of the newly acquired sound and the one with which it was previously replaced.
Correction of sounds l
,
l'
for various types of violations
Since the articulation of the solid sound l
more difficult than the articulation
of the
soft, then it is violated most often.
The defects are
varied, but here we will focus on the most characteristic ones.
Predisposing factors leading to incorrect pronunciation of the sound l,
may be the following:
- shortened hyoid ligament, which limits upward movement of the tip of the tongue;
- weakness of the tongue muscles;
- phonemic hearing disorders.
Absence of sounds l, l'
The speech of a child missing the sound l,
will sound like this: “Mouse veseo zhia, ka poukhu v uga spaa.” The mouse has cheese and sao, but everything to the mouse is about mao.”
Sound l
Preparatory stage. To correctly pronounce the sound l
you need to develop: raising the tip of the tongue upward;
raising the back of the back of the tongue upward, which can be achieved by practicing the sounds o
,
u,
and
s;
the ability to lower the lateral edges of the tongue and exhale a stream of air into the gap between the lateral edges of the tongue and the molars.
The solution to the last problem is the exercise “A hunter walks through a swamp.” The speech therapist says: “The hunter has big rubber boots and is walking through the swamp. It’s squelching under his feet like this.” Holding the wide tip of the tongue between his front teeth, he exhales air through his cheeks; while exhaling, he evenly hits himself on the cheeks with the index fingers of both hands, resulting in a squelching sound.
Sound production. When showing a child how to bite the wide tip of his tongue, they explain to him: “Make your tongue look like a pancake. Show me how you bite it with your teeth. Do it easily so that it doesn’t hurt, and watch how your tongue will lie motionless below your teeth, like a pancake on a plate. Now open your mouth and let your tongue remain as before. Do this several times in a row." (The child is practicing in front of a mirror.) Imitating an adult, the child will soon learn to lightly bite his wide tongue with his front incisors, then, opening his mouth, leave his tongue in the same position.
When the child has mastered this exercise, begin making the sound l
with the interdental position of the tongue (the so-called
interdental
Invite your child to make the sound a
at the moment when he releases his tongue after biting.
Let him repeat this exercise in front of the mirror 5-6 times, holding his tongue tighter with his teeth and increasingly alternating this movement with pronouncing the sound a.
Gradually, the pace of the exercise speeds up, and we will first hear the syllables
al, al, al,
then
la, la, la.
The speech therapist performs the exercise simultaneously with the child, but silently, so that he does not hear the sound l, but only sees the correct articulation and maintains the desired pace.
If a child hears that he makes the correct sound l,
and then returned to his usual pronunciation, you need to stop him and suggest doing the exercise more slowly.
In this case, the child’s attention should be drawn to the position of the tongue; “Watch your tongue, order it not to run away from you into your mouth, hold it with your teeth.” At a slow pace, he will be able, without interrupting the drawn-out pronunciation of the sound a,
to alternately bite and release his tongue.
This way he will get the syllables la, la, la.
Next, you should move your tongue to the tooth position, normal for this sound. The child is asked to lift his tongue by the upper incisors and, pressing it firmly to the alveoli, pronounce the syllables ly, ly, ly.
When combined with
the y
the l
sound acquires greater clarity.
Automation of sound l
begins with fixing it in syllables.
In this case, various gaming techniques are used, for example: imitating playing the balalaika, or singing songs to simple familiar melodies, or reproducing the sound of a bell, etc., the child repeatedly pronounces the syllables la, la, la,
then
ly, ly, ly,
then
lo, lo, lo,
then
lu, lu, lu.
Then the speech therapist draws pictures in the child’s individual notebook, the names of which contain the sound l
is in different positions: at the beginning of the word:
paw, lamp, bench, boat, palm, shovel, loto, curl, burdock, boat, crowbar, bow, moon, magnifying glass, beam loophole, lily of the valley, spoon, puddle;
in the middle:
saw, milk, bun, towel, tent, apple, soap, well, blanket, straw, spinning top, robe, balalaika, pin, stick, bun, dress, scarf, needle, doll, fork, strawberry, eyes, cap , cloud lightning, notepad, Christmas tree, ball, clown;
at the end:
table, chair, floor, oval, woodpecker, chalk, knot, trunk, corner, stake, channel, dump truck, torch, dome, pencil case.
The speech therapist or child comes up with sentences with practiced words. For example: Laika had a white paw. Mila put the lamp on the table. Alla gave Volodya a saw and a hammer. Klava drank milk and ate a bun. The ball fell from the chair to the floor. Paul sailed in a boat on the waves.
Sound l'
After automation l
hard soft sound is easy to imitate.
Showing articulation in front of a mirror, the speech therapist pronounces the syllables li, li, li
and draws the child’s attention to the fact that the lips are in a smile, the upper and lower teeth are visible, and the tip of the tongue knocks on the tubercles behind the upper teeth.
Having achieved the correct pronunciation of the syllable ,
they successively move on to the combinations
l
with
e, ya, ё, yu.
To consolidate
l',
words are selected in which this sound is at the beginning of the word:
swan, lazy, quinoa, lollipop, ice, husky, blade, ribbon, petals, fishing line, cake, ladder, bream, shower, lemon, ruler, fox, face;
in the middle:
album, orange, ticket, pancake, saucer, felt boots, cornflower, waffles, biscuits, dumbbells, strawberries, wicket, oilcloth, cranberry, wheel, cutlet, raspberry, butterfly, coat, stove, log;
at the end:
binoculars, jelly, blizzard, medal, moth, zero, stem, salt, poplar, tunnel, coal, beans, target, crack, sorrel, shawl, overcoat, dust, bed, furniture, feather grass, jacket.
Sentences are made with the learned words, for example: Lenya and Lena saw swans flying over the forest. Ilya and Leva were caught in a heavy downpour. Lilya was making an orange out of plasticine. Lucy has strawberries and raspberries on her saucer. Lyuba watered the leaves from a watering can.
Distortion of sounds l, l'
Interdental pronunciation of the sound l. With this type of pronunciation, the correct sound is heard, only its articulation is slightly changed: the tip of the tongue, instead of rising behind the upper incisors, comes out between the teeth. Interdental pronunciation l
used as a transitional stage when producing the sound
l
(see above).
Therefore, the correction of this defect is carried out in the same way as in the absence of the l sound.
However, it must be taken into account that to automate
l,
it will take more time for those children who pronounce interdentally not only this sound, but also others, for example:
t, dg n, s, z, c.
The nasal pronunciation of the sound l differs sharply from the correct one both in articulation and in hearing. The tongue touches the back of the tongue to the soft palate, and not the tip to the upper incisors, as happens with the correct pronunciation of the sound l.
In addition, the air stream passes partially or completely through the nose, as with the sound
n
.
Two indistinct sounds are heard: ng
. The child’s speech will sound like this: “Mouse vesengo zhinga, on the fluff in unggu spanga. The mouse is engga cheese and sango, but the mouse is all byngo mango.”
When correcting nasal pronunciation, first of all, it is necessary to develop the correct direction of the air stream: it should go through the mouth, and not through the nose.
The production and automation of sound with nasal pronunciation is carried out in the same way as in its absence.
Replacing sounds l, l'
other sounds (paralambdacisms)
Replacing sound l
sound
j. With this disorder, the tip of the tongue remains down instead of rising behind the upper incisors, and the middle part of the back arches upward instead of down.
The child says this: “The mouse is cheerful and alive, sleeping on the fluff of the eagles. The mouse is cheese and sayo, but everything is the same for the mouse.” Replacing sound l
the sound
u. With this disorder, the lips, rather than the tongue, take an active part in the formation of sound. Adults often find it difficult to tell how a child pronounces the sound l,
because by stretching his lips forward, as with the sound
u,
he quickly moves on to the next sound in the word and the listener does not have time to notice how the sound is pronounced.
But if you invite your child to make the sound l,
it will be easier to notice the movements of his lips.
If you hold the child’s lips in the corners of his mouth with his fingers so that they are motionless, you can easily make sure that he cannot pronounce the sound l at all.
With this replacement, the child’s speech sounds something like this: “Mouse veseuo jiua, on the fluff in uguu spaua. The mouse is cheese and sauo, but everything to the mouse is mauo.” This deficiency, if not corrected, often remains for life.
Replacing sound l
sound
s. With this type of incorrect pronunciation, the back of the tongue is raised and the tip is lowered. Children do not notice that they are replacing the sound, and adults often believe that the sound l
is skipped. The child says: “The mouse is happy and alive, on the fluff of the bed.” The mouse is cheese and cheese, but everything is too much for the mouse.”
Replacing sound l
sound
in. With such a replacement, the tongue does not take part; the lower lip moves towards the upper incisors. Children and adults often believe that this is not a speech deficiency, but only an unclear pronunciation of the sound l
. With this replacement, we hear: “The mouse is cheerfully alive, on the fluff of the ugwu spava. The mouse has cheese and savo, but everything was mavo for the mouse.”
Replacing sound l
with the sound
g. In this case, the tip of the tongue does not rise to the upper incisors, but falls and is pulled away from the lower incisors, the back of the back of the tongue rises and rests against the soft palate, instead of just rising.
The child’s speech sounds like this: “The mouse has a lot of fun, on the fluff in the uggoo spaga. The mouse era is cheese and sago, but everything about the mouse is old mago.” Correction of paralambdacisms at the preparatory stage is carried out in several directions at once: they are taught to distinguish the sound l
and its substitute, be aware of the difference in their articulation, clearly perform the tongue movements necessary for the correct pronunciation of the sound
l.
But in some cases, exercises for the tongue and lips have their own characteristics:
— when replacing l
On
j, the child is taught to hold the tip of the tongue behind the teeth, pressing it firmly against the upper incisors, lower the middle part of the back of the tongue, and raise the back. In order for the tongue to take this position, the child is asked to insert the tip of the tongue between the front teeth and say drawn out, or
with the mouth open, place a round plastic tube on the middle part of the tongue, and lift the tip of the tongue behind the upper incisors;
— when replacing l
First
all , it is necessary to bring to the child’s consciousness that the lips should not move. To do this, he is asked to look in the mirror at his lips while repeatedly pronouncing the syllable la.
Then the adult himself pronounces this syllable and draws the child’s attention to the fact that the lips do not extend forward, the tongue is visible all the time - it descends from top to bottom. The child is told: “Your lips are naughty. You want them not to stretch forward, but they do it their own way. Let's teach them to obey. We command our lips: stretch forward! (The child easily performs the movement that is familiar to him.) Now stretch your lips as if you were smiling (this also does not make it difficult for the child). You see, the lips have become obedient because you told them what they should do.” The exercise is repeated several times until the child learns to easily switch from one movement to another at a fast pace. “Now let’s work with the tongue. Look what my tongue will do,” (the speech therapist lifts the tongue by the upper teeth, presses its tip tightly, then lowers it. The lips are always in a smiling position). Do the same.” The child repeats the exercise several times, and the teacher makes sure that he does not bend the tip of his tongue inward;
— when replacing l
It
necessary to slow down the movements of the lower lip.
To do this, the child is taught to first lower it, exposing the teeth, and hold it in this position for a count of 3 to 5, then lift it to the upper teeth. These movements are repeated several times. If the child does not succeed, use mechanical assistance: lower and raise the lower lip with the index finger placed under it: - when replacing the lip
in
d the child is shown what are the errors in his pronunciation and how it differs from correct articulation.
The speech therapist says: “Say la, la, la...
(the child pronounces “ha”, “ha”, “ha”).
See how far your tongue has gone? Look where I have it. It is pressed against the upper teeth. Do the same. Say y,
but don’t lower your tongue, but hold it behind your teeth, like this.”
Staging and automation of sound l
are carried out as in his absence.
If, with lambdacisms, correction of the sound l
ends with the stage of automation, then with paralambdacisms it is necessary to carry out a complete differentiation (in an isolated position, syllables, words, phrasal speech) of this sound and its substitute.
Topic 9. Defects of palatal sounds (k, k'; g, g'; x, x'; u(j))
and their correction
Disadvantages in the pronunciation of sounds k
and
k'
are called kappa c and zma,
g
and
g'
- gammatism,
x
and
x'
- hitism.
Those types of defects that are associated with the replacement of these sounds with some others are called paracappacism, paragammatism, parachitism. Lack of pronunciation of the sound th (j) is called
Articulation of
is as follows. The position of the lips depends on the following vowels. Some distance is maintained between the upper and lower incisors. The tip of the tongue is lowered and significantly removed from the lower teeth, and the back of the back of the tongue closes with the palate. At the moment the sound is pronounced, the bow between the tongue and the palate explodes, clearing the way for the air passing behind under pressure, which bursts out with a characteristic noise. The soft palate is raised and closes the passage to the nose. The vocal folds are open (Fig. 8).
Sound g
according to the mechanism of its formation, it differs from sound
to
only by the closure and subsequent vibration of the vocal folds already at the moment preceding the explosion (Fig. 8).
Feature of the articulation of the sound x,
what distinguishes it from the sound
k
is that the back of the tongue does not completely close with the palate, leaving a gap in the midline, through which a stream of exhaled air passes causing the noise inherent in the phoneme
x
(Fig. 8).
Soft sounds k', g', x'
(Fig. 9) differ from paired hard palates by moving the occlusion or fissure formed by the tongue and palate forward, to the middle part of the hard palate.
There are three main types of kappacism. The peculiarity of the first type is that instead of sound
a characteristic soft guttural click is heard. It occurs as a result of the fact that the vocal folds close tightly, the action of the respiratory muscles under them creates increased air pressure, after which the closure explodes and air noisily breaks through the glottis.
The second type includes paracapacism in the form of replacement of sound with
to the sound
t
(“tapusta”, “reta”, “paut”).
In the third case, the explosive sound
is replaced by the fricative
x:
(“khapusta”, “reha”, “pauh”), which again characterizes the defect as paracappacism.
An anomaly in the structure of the speech apparatus, which predisposes to the occurrence of cappacism, is the irregular shape of the hard palate, when it turns out to be too narrow and high, making it difficult to form a dense lingual-palatal stop.
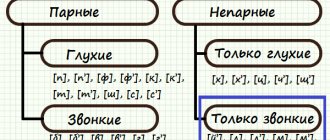
Phonetic characteristics of the sounds [L] and [L']
The sound [L] is a consonant, transitive, oral, anterior lingual. When it is articulated, the lips assume a half-smile position and the teeth open. The tongue is saddle-shaped, with a narrow tip resting on the base of the upper incisors. The edges of the tongue form a gap with the lateral teeth through which air escapes. The vocal folds are brought together and vibrate to form the voice. This is the only phoneme in the Russian language that is pronounced in a narrow language.
When pronouncing [L'], the tip of the tongue is raised towards the alveoli and is more tense. The anterior-middle sections of the back of the tongue are close to the palate, giving softening (palatalization).
Position of the tongue when pronouncing the sound [L]
Types of lambdacism
The hard [L] is the most complex articulatory, therefore it is violated much more often than its soft pair. The following types of lambdacism are described in speech therapy:
- Bilabial (labial-labial).
The most common phonetic defect. The tongue is not involved in articulation; the sound is formed by bringing the lips together, resulting in something similar to English [W]. - Labial-dental.
The lower lip comes closer to the upper teeth, as a result of which a sound similar to [B] is heard. - Interdental.
The tip of the tongue is inserted between the lower and upper incisors, but the interdental [L] does not differ by ear from the correctly articulated one. - Nasal.
The back of the back of the tongue closes with the soft palate, while the air exits through the nasal cavity, making the sound reminiscent of [N] or the combination “NG”. - Side.
Pronunciation is accompanied by swelling of the cheeks (sometimes on one side) and additional noisy sounds. Often combined with lateral rhotacism and sigmatism of sibilants. - Softened.
Instead of a hard phoneme, its semi-softened version is pronounced.
In addition to the listed types of lambdacism, sonor [L] may be completely absent in speech. There is also a lower variant of pronunciation, in which the tip of the tongue does not rise upward. In the latter case, the sound is not distorted, so such a violation may not be corrected. Paralambdacisms include replacements of [L] with [Н], [У], [В], [J], [Р].
Treatment of lambdacism at the multidisciplinary center “Academy of the XXI Century. Speech.Intelligence”
When faced with such a problem as lambdacism, there is no need to be ashamed of it, much less let it take its course. Modern treatment methods, qualified specialists, an individual approach to each client and a comprehensive examination of the multidisciplinary center “Academy of the XXI Century. Speech.Intellect” will help to cope with this task. Our main specialist and project manager, Danilkina Margarita Yurievna, is a hereditary defectologist, a famous speech therapist, neuropsychologist, oligophrenopedagogue, specialist in the development of intelligence, rehabilitation, diagnosis and correction of developmental disorders in children and adults, the author of unique methods for the development of children in conditions of sensory-emotional play expansion and advanced development, professor, full member of the European Academy of Natural Sciences (Hannover).
There are no unsolvable problems, there are just lazy specialists. Professor Danilkina Margarita Yurievna has many scientific works on very complex diagnoses. Giving lectures at various universities around the world and conducting practical work. New techniques allow you to achieve amazing results.
Contact us at the center and you will see that together we can handle mountains.
Diagnostics
The task of determining the causes and type of lambdacism is implemented during speech therapy diagnostics. If it is necessary to clarify the medical aspects of the pathology, consultations with a pediatric dentist, maxillofacial surgeon, neurologist, or otolaryngologist are prescribed. To study speech status, the following is carried out:
- Examination of peripheral speech organs.
The speech therapist visually assesses the structure of the tongue, palate, lips, and pays attention to muscle tone. The child is asked to perform certain exercises that allow him to judge the mobility of the speech organs, the accuracy and switchability of movements. As part of such an examination, possible causes of lambdaism are established and a diagnostic hypothesis is put forward. - Analysis of phonemic hearing.
Necessary for the purpose of differentiating lambdacism and paralambdacism. To test speech hearing, speech therapy techniques of repetition, naming, and demonstration are used. Phoneme discrimination is tested in syllables and words. - Assessment of the phonetic side of speech.
At this stage, the pronunciation of all sounds is checked: the type of lambdaism is determined, and accompanying sound defects are identified. Based on the examination results, a plan and sequence of correction are outlined.
Articulation gymnastics
Correction
Health care
The participation of medical specialists may be required in case of lambdacism caused by dental problems, neurological pathologies (cerebral palsy), or hearing loss. Thus, with a shortened frenulum, in some cases, preliminary frenuloplasty is necessary, and with a cleft palate, uranoplasty is necessary. Hearing loss requires adequate selection of hearing aids. In case of a violation of muscle innervation, speech therapy work is preceded by a complex of medication, physiotherapeutic treatment, and massage.
Speech therapy assistance
Before starting to establish standard sound pronunciation, preparatory work is carried out to form the correct articulatory posture and develop phonemic hearing. At the first stage of correction of lambdacism, the following speech therapy techniques are used:
- Articulation gymnastics.
Includes exercises for developing the circular muscles of the lips (“Smile”, “Tube”), muscles of the tongue (“Needle”, “Watch”), stretching the hyoid ligament (“Horse”, “Mushroom”), developing the upper position of the tongue (“Painter” , “Swing”, “Turkey”), etc. It is also necessary to pay attention to the correct speech exhalation (exercise “Steamboat”). - Practicing basic sounds.
The supporting phonemes for [L] are [T] - gives the correct position of the tongue and [Y] - ensures the correct supply of the air stream. - Speech therapy massage.
Indicated for insufficient tongue mobility, weakness of the tip and lateral edges, spasticity of the back. Typically, such problems are observed with dysarthria. The most effective in this case is probe logomassage.
Sound production begins after completion of the preparatory stage. For various forms of lambdacism, differentiated methods and techniques are used: by imitation, based on basic sounds, using staged probes.
As soon as the sound [L] is received, they move on to consolidating it in syllables (direct, reverse, with a combination of consonants), words, phrases, stories. The differentiation stage is only necessary in cases of paralambdacity. The duration of correctional speech therapy sessions depends on the cause and mechanism of lambdaism, the presence of other phonetic defects that need correction.
Articulation gymnastics
Therefore, in order to correctly reproduce the sound [l], it is necessary to develop the tongue and lips. Articulation gymnastics will help us with this. [L] is the sound of the upper rise of the tongue, so I advise you to “warm up” the tongue from early childhood with such amusing exercises as “horse”. Simple clicking in a playful way trains the muscles of the tongue very well. Unfortunately, many children who come to me in first grade do not know how to make a “horse” at all. Therefore they do not have most of the top rise sounds. The tongue lies like a dead weight at the bottom of the oral cavity and cannot touch the palate without the help of the lower jaw, producing a characteristic clicking sound. Gradually, the kids and I begin to move the tongue as best we can. Already a month after such daily “twitching”, a full-fledged clicking sound and the correct “horse” emerge, that is, the movements of the tongue should be autonomous, while the lower jaw is motionless. I also recommend starting from the age of one year to practice such an upper lifting exercise as “tasty jam”, licking the upper and then the lower lip with the tip of the tongue, while simultaneously developing the orbicularis labii muscle.
So, what exercises do we need to make the sound [l]:
- "Smile";
- "Smile-pipe";
- "Shovel";
- "Delicious jam";
- "Hedgehog";
- "Swing";
- "Watch";
- “Let’s brush our teeth with our tongue”;
- "Painter";
- "Horse";
- "Fungus";
- "Turkey";
- "Sail";
- "Steamboat".
I would especially like to dwell on the last two exercises, they are aimed specifically at the correct pronunciation of [l].
"Sail"
– this exercise helps strengthen the muscles of the tongue, training its upper rise. The mouth is wide open, the tongue is straight (no need to wrap it in a roll), rises up and, touching the sharp tip with the upper alveoli, stands exactly behind the upper teeth, first on a count of 10, then from time to time increasing the “stand” by ten points, bringing up to 40.
"Steamboat"
– staged exercise for the sound [l]. Stick the flattened tongue out of the mouth, biting the tip with your teeth, spread your lips into a smile, pronounce for a long time: “Yyyyyyyyyyyyyyyyyyy”, which will smoothly move to “Yyyllllllllllll”.
Read also:
Speech disorders in children
Several ways to develop speech