Speech therapy examination
In a speech therapy examination of a child of the 2nd and 3rd year of life, only the main directions of the examination and those stages of age-related development of child speech are highlighted, without which the idea of a young child will be insufficient.
The proposed method of speech therapy examination is based on the scheme of the systemic development of normal child speech compiled by N.S. Zhukova based on factual materials from the book by A.N. Gvozdev “Issues of studying children's speech” (1961), as well as on the diagnosis of neuropsychic development of children of the 2nd and 3rd year of life, compiled by K.L. Pechora and G.V. Pantyukhina (1979).
Before starting the examination, it is necessary to accurately establish the child’s date of birth, since tasks are initially offered from the age period that corresponds to the actual age of the child. If the child’s age is between two age periods, then the initial tasks are the tasks of the closest younger period. After presenting the child with all the tasks from the initial age period and assessing their performance, depending on the results obtained, they move on to tasks either from an older age period or from a younger age period. The normal development of a child of the 2nd year of life is considered to be the formation of speech within one quarter:
- 1 year 1 month 1 year 3 months,
- 1 year 4 months 1 year 6 months,
- 1 year 7 months 1 year 9 months,
- 1 year 10 months 2 years.
In the 3rd year - within six months:
- 2 years 1 month 2 years 6 months,
- 2 years 7 months 3 years.
A speech therapy examination includes the collection of data on the early pre-speech development, pre-speech and speech development of the child up to the time of the examination (analysis of extracts from the history of development, analysis of the stage epicrisis in the history of development, etc.). Further, the structural features of the skull, face, the presence or absence of craniofacial asymmetries are noted in various emotional states of the child: during laughter, screaming, crying, frowning, squinting, etc. The formation of voluntary movements in the facial muscles is noted: the ability to frown, raise eyebrows, puff out cheeks.
An examination of the articulatory apparatus includes an assessment of the structural features of the articulatory organs, involuntary movements of the articulatory organs during eating (biting, chewing, swallowing), during facial reactions, speech reactions, during wakefulness, play, the formation of the level of voluntary movements (by display and word with 1 year 6 months).
Muscle tone in the organs of articulation is assessed jointly by a speech therapist and a neurologist.
Further, in the speech therapy examination, the features of the child’s respiratory system, features of the general sound of speech and voice are noted.
The next stage of examination of a child of the 2nd and 3rd year of life is an examination of the formation of speech understanding. In the 2nd year of life, the child’s understanding of speech and generalization function improve, the conceptual vocabulary expands, and connections between objects, actions and their verbal designations develop more intensively. From 1 year 6 months, the child begins to understand adult speech that is not supported by the situation.
In the 3rd year, the understanding of the speech of others changes significantly: the child begins to understand temporary relationships. You can talk to him not only about this moment, but also about the past (what happened yesterday, what they collected in the forest in the summer, how they decorated the Christmas tree, etc.) and about the future (where he will go tomorrow, what he will do on a walk, etc. .d.). A child can understand events in an adult’s story that he himself did not perceive. The child begins to understand some grammatical relations: prepositional-case relations, suffixal relations, prefixal relations, as well as some categories of noun, verb, adjective.
The section “Active Speech” notes the age-related development of the lexical and grammatical side of speech, the assimilation of parts of speech, the formation of the syllabic structure of words and the sound side of speech.
The level of formation of auditory attention and phonemic hearing is important for speech development.
To examine auditory attention, special games are played: “Guess what sounds,” “Guess who called you.”
When examining phonemic hearing, the ability to distinguish and recognize words that sound similar is tested.
In the “Fine motor skills of the hands” section, anomalies in the structure of the hands, the position of the fingers of the hand, the movements of pronation - supination of the hand, the formation of differential grips and the opposition of the fingers are noted.
The speech therapy examination ends with an analysis of the data obtained in the form of a speech report.
We distinguish between normal child development and development ahead of one to two epicrisis periods (one to two quarters, half a year), which is a physiological norm, development ahead of three or more epicrisis terms (three quarters or more) and delayed development, which includes includes a delay in the pace of development and a delay in development itself.
A delay in the rate of development suggests that the child lags behind his normally developing peer only in terms of the timing of the formation of mental processes and speech, that the delay is due to a slowdown in the rate of maturation of brain structures and their functions in the absence of qualitative changes in the central nervous system (Zhurba L.T., Mastyukova E. M., 1981).
Developmental delay suggests that the child’s development of mental processes and speech is qualitatively deteriorating, as well as the fact that he lags behind his normally developing peers in terms of the timing of the formation of these processes.
According to the degree of severity, delayed development is divided into mild delay, significant (medium) delay, and severe (severe) delay.
A mild developmental delay is indicated by the fact that the formation of age-related skills is delayed by no more than one to two epicrisis periods (one to two quarters, one half-year). At the same time, there is a tendency towards a gradual reduction in the time deficit as it grows and corrects.
With a delay of moderate severity (a delay of two to four epicrisis periods or two to four quarters, or two half-years), the time deficit in the development of age-related skills does not tend to decrease, and sometimes increases as the emerging functions become more complex. Emerging skills are deficient or have qualitative features.
Severe developmental delay is characterized by a pronounced temporary deficit in the development of age-related skills, exceeding five to six epicrisis periods (four quarters and two half-years), and a steadily increasing lag as the child grows. Age-related functions either do not appear or are rudimentary and grossly altered.
Speech therapy examination
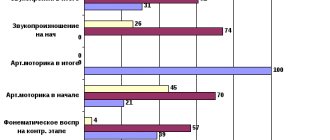
LogoKot presents a system for examining children with speech disorders. The program includes the following areas of examination:
- Sound pronunciation survey
- Examination of the structure of the articulatory apparatus and Examination of articulatory motility
- Phonemic Awareness Test
- Examination of the syllable structure of a word
- Vocabulary Survey
- Examination of grammatical structure
- Examination of coherent speech.
The Internet program provides for processing the results of the examination, calculating the points scored by the child as a result of the examination, and issuing a speech therapy report. The results of the examination are documented in a speech card. The speech card is saved in LogoKot in the speech therapist’s personal account. The speech therapist can then save the speech map to his computer (instructions on how to save the web page are available here). The speech card can be easily processed to display other specialist documents: characteristics of the child, referrals for MPT, etc.
The program uses a leveled approach to diagnosing speech underdevelopment. The scores that a child gains as a result of the examination indicate the state of speech development. The program, based on the results of the points scored, offers options for a speech therapy conclusion. The teacher can reasonably write a conclusion, and also monitor the results of correctional work during further examinations.
1. Examination of sound pronunciation:
In the section “Survey of sound pronunciation” the following groups of sounds are examined: whistling (s, s'z, z', ts), hissing (sh, zh, h, sch), sonorant (l, l', r, r), back-lingual ( k, g, x).
The child is asked to name the pictures; if he names the sound in the pictures correctly, the speech therapist continues examining other sounds and presses the “no error” button. If the child makes a mistake (the sound is missing, replaced or distorted), then the speech therapist presses the “error” button and continues the examination.
When examining sound pronunciation, two options are possible: the sound is impaired / the sound is not impaired. Each incorrectly pronounced sound is scored 1 point.
2. Examination of articulatory motor skills
The identification of the characteristics of articulatory motor skills is carried out in the process of the child performing certain actions at the direction of the speech therapist. Includes:
- Study of lip mobility.
- Study of tongue mobility.
- Study of lower jaw mobility.
- Study of the mobility of the soft palate.
When performing tasks, difficulties in the movements of the articulatory organs are diagnosed: obvious impossibility, significant limitation in the range of movements, a tendency to constantly hold the tongue in a “clump” in the depths of the oral cavity, difficulties in changing the given position of the speech organs, tremor, hyperkinesis, synkinesis, slowing down the pace with repeated movements. When analyzing the state of articulatory motor skills, the following parameters can be taken as a basis:
- Movements of the articulatory apparatus: active, passive.
- Range of motion: full, incomplete.
- Muscle tone: normal, flaccid, overly tense.
- Accuracy of movements: accurate, consistent, inaccurate, no sequence of movements.
- The presence of accompanying and violent movements.
- Rate of movement: normal, slow, fast.
- Duration of holding articulators in a certain position.
Based on the results of the examination of articulatory motor skills, the level is determined.
3. Examination of the structure of the articulatory apparatus
Includes:
- Lip examination.
- Dental examination.
- Bite examination.
- Language research.
- Examination of the hard and soft palate.
- Examination of the lower jaw.
The examination reflects the structural features of the articulatory apparatus: normal, mild deviations, gross deviations.
4. Phonemic Awareness Test
Includes:
- Study of the state of physiological hearing.
- Study of differentiation of non-speech sounds.
- Study of the discrimination of syllables and words with oppositional sounds.
- Study of phonemic analysis and synthesis (in children over four years old).
5. Examination of the syllable structure of a word
The examination of the syllabic structure of a word is carried out according to Markova classes.
6. Vocabulary examination
Vocabulary examination is carried out according to the following parameters:
- Study of generalizing concepts.
- A study of occupational understanding.
- Exploring the understanding of shapes and colors of figures.
- Study how a child can form words.
- Other
7. Examination of grammatical structure
The examination of grammatical structure is carried out according to the following parameters:
- Research on the formation of multiple forms.
- Study of the formation of diminutive forms.
- Study of the use of prepositions.
- Study of sentence construction.
- A study of the formation of nouns in oblique cases. Prepositional case forms.
- Study of numeral-noun agreement.
- 7. Research on understanding the names of baby animals
8. Examination of coherent speech.
The story is assessed taking into account:
- its correspondence to the depicted situation (presence of distortions, additions);
- integrity (the presence of all semantic links);
- correct sequence;
- smoothness of presentation: conveys the content without stops, long pauses, additional words (for example: “Well, what’s next?”, etc.);
- understanding the content of what is being presented;
- completeness of the retelling (presence of omissions);
- the nature of language design (grammatical correctness of sentences);
- the method of performing the task (independently or with the help of an experimenter);
Rationale for speech therapy report
Based on the results of the examination and based on the number of points scored by the child, a conclusion is given about the state of speech development of each child. As a result of a complete examination of the child, the following conclusions may be made:
First level (low, 56-67 points) – General underdevelopment of speech OHP level I. Speech as a communicative function is absent.
Second level (below average, 43-55 points) – General underdevelopment of speech OHP level II. Speech activity has increased, but speech does not fulfill its role as a communicative function.
Third level (average, 21-42 points) – General speech underdevelopment OHP level III. The speech is understandable, however, there are lexico-grammatical, phonetic-phonemic disorders and, in general, unformed coherent speech.
Level four (above average, 5-20 points) – Phonetic-phonemic underdevelopment - along with a violation of the phonetic side of speech, there is also underdevelopment of phonemic processes: phonemic perception (auditory differentiation of sounds), phonemic analysis and synthesis, phonemic representations. Perhaps, most often as a result of speech therapy: mild general speech underdevelopment (GUSD) or general speech underdevelopment GSD level IV; In the absence of sound pronunciation disorders, the following conclusion is possible: lexico-grammatical underdevelopment of speech (LGNR - children have normal sound pronunciation, phonemic processes are relatively preserved (most often as a result of speech therapy), but there is a limited vocabulary, a violation of the grammatical structure of speech).
Fifth level (high, less than 4 points) – Normal speech development is possible. In the presence of impaired sound pronunciation, a phonetic speech disorder (FSD) or a violation of the pronunciation of individual sounds (NPOS) is possible.
This form of recording the results obtained, a level approach to assessing the results of the study, allows you to correctly draw a conclusion about the state of the child’s speech development, and reliably monitor the dynamics of correction of the speech defect not only in one specific child, but also in the group as a whole.
The results of the examination are documented in a speech card.
Log in to the service to get full access to the knowledge base