Article:
By the age of three, most children are already quite independent, they have an idea of the world around them, are armed with some knowledge about objects and their properties, and a child’s speech at 3 years old contains a sufficient number of related words and sentences.
After all, they have tested a lot of their knowledge in practice, that is, children have tried out from their own experience how to manipulate objects in their environment, and now they can talk about it with understanding. A child's speech development at 3 years of age has a particularly wide range for different children of the same age. Some do not experience any difficulties in their statements, are sensitive to the slightest deviation from the norm in the speech of the adults and peers around them, and show interest in the sound analysis of words. At the same time, other children had just begun to construct sentences more or less correctly, and their speech was very far from perfect.
Features of speech development in children 3–4 years old
At this age, children's speech continues to actively develop. Children of the fourth year of life begin to draw conclusions and can reason about objects and the phenomena surrounding them. The child is interested in the world of people and things, he is interested in communicating with loved ones and with strangers. The time has come for questions, the answers to which the child, due to his age, is sometimes not able to listen to the end.
Active and passive dictionary
The development of speech for children 3–4 years old leads to the fact that the number of words that children use in speech (active vocabulary) doubles: from 1 thousand words available to them by the age of three, to 2 thousand by the end of the third year of life . Moreover, they not only use them, but inquisitively listen to the meaning of words, and even create their own. “Who called a cat a cat and a hippopotamus a hippopotamus?” Children play with the word, tasting it, rhyming and changing it, coming up with incredible combinations of sounds: milk, toloko, far, coloko; slam, slam, slam, slam.
Long new words, incomprehensible in content, can be pronounced distorted (lipestricism - electricity, lisipede - bicycle), syllables and sounds are often rearranged in them (pervyi - first, gamazin - shop). Combinations of two consonant sounds in a row continue to cause difficulty in pronunciation. In order to pronounce them correctly, the child inserts a vowel sound between them (zinayu - I know), or simply does not pronounce one consonant sound.
Children can already name the details of objects, distinguish externally similar objects, for example, a cup-mug, a tiger-lion. By the age of three, most children should already be able to easily distinguish the animals in the picture below (show it to your child and check):
When learning new words, children of this age establish semantic connections between objects, actions and their names. They begin to think meaningfully about the vocabulary of their native language. However, children's speech is not yet developed enough for full communication. If at the everyday level the baby still has enough mastered words, then they are not enough to retell a long fairy tale or describe a memorable event.
Speech grammar for three-year-old children
The speech of a four-year-old baby consists of phrases. On average, there are 3-4 words in a sentence. At the age of four, they become common, and complex constructions begin to appear - compound and complex sentences. For example: “the doll wants to eat, I’ll make soup,” “when spring comes, the birds fly.”
Children can use singular and plural homogeneous members in phrases. For example, “I draw flowers and clouds”, “the mouse jumps and laughs”. Nouns and verbs begin to give way to their positions; more and more adjectives, adverbs, pronouns and numerals (one, two, three, first, second, third) are found in speech.
But the speech of a 3-year-old child is still imperfect; it is difficult for him to form the plural of many nouns, for example, trees, mouths, sleeves. In coordinating adjectives with nouns, he can also make mistakes, for example, “ripe apple”, “bright sun”.
Often in the speech of children there are incorrect case endings, and the change of the verb in persons and numbers suffers. For example, “I see trees”, “I have a lot of candy”, “children are riding bicycles”. Show the picture below to your child and check this point:
Sound pronunciation
The child grows - his articulatory apparatus becomes stronger, the movements of the tongue, lips, and lower jaw become more accurate and coordinated. A stronger tongue allows you to correctly pronounce previously softened consonant sounds: malyako - milk, syadik - sadik. Long words of 3–5 syllables, as well as words with combinations of two consonants such as bread, class, bottle, are easier to learn.
Most often at this age the following sound pronunciation disorders occur:
- Replacing hissing sounds with whistling sounds: sapka - cap, nozik - knife;
- Unclearly pronounced sound ts, ch: tsyplenok - chicken, prints - prince, tai-chai;
- Absence in speech of the sounds l, r or their replacement with the sounds y, v, softened l: liba - fish, yodka - boat, vozhka - spoon.
If you notice these disorders in your child, you should not worry, but you should consult with a speech therapist. He will always tell you whether this is the age norm, which does not yet require the intervention of a specialist, or not. Although, we must pay tribute, already at this age there are children whose sound pronunciation has practically no defects.
Speech development at 3 years allows for rearrangements and omissions of syllables in polysyllabic words such as hello, please, purple. Such pronunciation deficiencies are successfully overcome by the end of this age period.
The intonation expressiveness of speech is growing - children can imitate adults, adding very expressive notes to the reading of poems by heart and to stories from their own experience. Adjusting the rate of speech and its volume is not always available to children of the fourth year of life. They may speak very quietly, especially when talking to people they don't know. When the impressions of some significant event are too great, the child can talk about them “excitedly,” hesitating and hastily pronouncing words.
A very valuable quality appears - attention to one’s own speech and to the speech of others. Children begin to notice pronunciation deficiencies made by their peers, but less often - their own.
Connected speech
A three-year-old child is not yet able to logically and coherently talk about what he saw, what interested him, or completely retell the content of a work of art read to him. Children of this age are still unable to deliver a monologue on any topic without additional questions. Children's statements are not developed, the phrases are simple and not always connected with each other.
Children cannot compose a coherent story from a picture. They can only list the objects depicted on it and the actions performed by the characters in the image. “There’s a bunny here. He eats carrots. His mother is there. She sits and watches."
Children of this age easily remember and enjoy reciting poems and nursery rhymes that are understandable in content. They can repeatedly listen to the same fairy tale, and then retell its content almost word for word, and the content of some words may be completely incomprehensible to them (bast hut, tar barrel).
Speech examination of preschool children
Lyubov Alekseevna Aksenovskaya
Speech examination of preschool children
Speech examination of preschool children
Prepared by teacher-speech therapist MADOU d/s No. 55 “Fairy Tale”
combined type GOSH
Aksenovskaya L. A.
Examination of children's speech by group teachers.
Before starting work on teaching correct pronunciation, the teacher gets acquainted with the speech of each child in his group. The survey is carried out twice : in the fall, to properly plan the work for the year, and in the spring, to sum up the results.
When planning an examination , the teacher must clearly understand what he needs to identify in the child’s speech , know how to conduct the examination , what material to use, how to format the results and what conclusions to draw. When examining a child’s speech, the teacher pays attention to the state of sound pronunciation, vocabulary and phrasal speech . If there are dictionary violations (omissions, rearrangements of syllables, sounds)
and phrasal
speech (does not coordinate words in a sentence)
or serious deficiencies in sound pronunciation, you should get acquainted with the data on the child’s health, since the development
of speech is closely related to its psychophysical development.
Various infectious diseases in the first three years of a child’s life, especially diseases associated with nutritional disorders (dyspepsia, dysentery, etc., retard the growth and development of the entire organism, including speech . The success of working to educate correct pronunciation in the weakened and developmentally delayed children largely depend on strict adherence to the regimen prescribed by the doctor.
When developing correct sound pronunciation in children of the speech of surrounding adults plays an important role .
Therefore, the teacher must certainly know how the child’s family members speak in order to involve only those who speak correctly in sound pronunciation classes with the child at home.
First, the teacher studies the child’s speech in classes, in games with children, where he can identify his vocabulary, ability to construct a phrase, speech (very fast or slow, existing speech (stuttering, delayed speech development, etc. )
.
Then he conducts an individual examination , during which he identifies the child’s speech . the examination when there are few children (during their arrival and departure home)
.
Sometimes during an individual examination it is limited to asking the child to repeat individual words or sounds after the teacher. This does not give an idea of children's independent speech . By imitating the teacher, the child often pronounces sounds better than in independent speech .
Experience has shown that it is also impossible to check sound pronunciation by limiting yourself to listening to a poem read by a child, since in a poem memorized from the words of an adult, he pronounces sounds better than in ordinary speech . In addition, the poem may be missing sounds that need to be checked. Therefore, the examination is carried out using special material, which should be in each group.
Material for examination .
The material is selected by the teacher and formatted correctly. To examine sound pronunciation, you need to have object pictures for certain sounds. Often this material is presented in the form of albums. On one page of such an album there are usually 6 – 9 pictures. But when they are offered to a child, his attention wanders. In addition, even if it is clear how the child pronounces a sound, all pictures are watched to the end, since it is interesting to him. In addition, pictures pasted in the album cannot be used in further work. Therefore, it is more advisable to put pictures in envelopes. The teacher selects pictures so that each of being examined is at the beginning, in the middle and at the end of the word, since the sound is not pronounced the same in different positions. Pictures should be colorful and accessible both in content and execution.
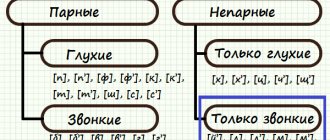
Pictures are selected to test the following groups of sounds:
1 – voiced consonants V, B, D, G
2 – whistling S, S, Z, Z, C
3 – hissing Sh, Zh, Ch, Shch
4 – sonorous L, L, R, R
5 – sound Y at the end and beginning of a syllable
For each sound position in a word (beginning, middle, end)
The teacher selects at least three pictures in order to be able to hear and record how the child pronounces this sound. The size of the subject pictures is 10 x 10 cm. Smaller pictures can be pasted onto cardboard of the accepted size.
When selecting material, you need to remember that the voiced consonant sounds Z, Zh, V, B, D, G at the end of words and in the middle, if followed by a voiceless consonant, are deafened, i.e. they are pronounced as their corresponding paired voiceless sounds: Z like C (watermelon, birch tree, F like W (knife, spoon, V like F (carrot, bench, B like P (pillar, box), D like T (grandfather, boat, G like K (arc, claws)
.
Therefore, you should not take pictures where these sounds are at the end or middle of the sound, when they are followed by a voiceless consonant. It is necessary to select pictures so that these sounds are located between two vowels (knives, watermelons)
or before sonorant, voiced consonants
(scissors)
.
To check a child’s vocabulary, no special material is selected, since this is almost impossible to do. But when naming object pictures while checking sound pronunciation, you should also take into account the state of the dictionary, see if the child makes rearrangements in words, omissions of syllables, or abbreviations of words. Basically, the teacher finds out the state of vocabulary and phrasal speech in classes in different sections of the program. The teacher can clarify the construction of sentences, the correct use of prepositions, and the coordination of sentence members in gender, number, and case using plot pictures. The pictures are selected so that they can be used to make sentences of two, three, four or more words. They must be given in order of increasing difficulty .
Conducting an examination .
Having prepared the material, the teacher begins an examination of sound pronunciation . He notes not only the absence or replacement of sound, but also its distortion, any inaccuracy in pronunciation. When it is not possible to establish how the child pronounces a sound, but the auditory pronunciation differs from the correct one, the teacher notes that the sound is not pronounced clearly. Sometimes a child, naming pictures for a given sound, cannot pronounce it correctly in a word. In this case, the teacher invites the child to pronounce the sound by imitation. He says: “A mosquito flies and rings - z-z-z. Call too, like a mosquito"
. If a child, imitating a mosquito, pronounces the sound Z correctly, this means that isolated pronunciation of the sound is possible, although the child has not yet introduced it into speech. In this case, it is necessary to consolidate this sound, that is, gradually introduce it into words, phrases, nursery rhymes, etc. If the child replaces the sound with another or pronounces it distorted, it means that he does not yet have this sound. In this case, you must first evoke the correct sound and only then introduce it into speech.
When examining children's speech, the teacher pays attention to the pace of their speech , clarity, correct pronunciation of words, and sonority of the voice. If there are any shortcomings, they should be noted.
Children who have not yet developed phrasal speech or often have incorrect construction of sentences, violations in the agreement of words in gender, number, case, or control, are examined using plot pictures. With them
With the help of the teacher, he clarifies errors encountered in the child’s formation of phrases. During the examination, you must not repeat sounds, words, or phrases pronounced incorrectly by the child. This not only traumatizes him, but also helps to reinforce the incorrect pronunciation.
Registration of survey .
When conducting an individual examination , the teacher writes down all the children's in a notebook indicating the date of the examination . In the notebook, one to two pages are allocated for each child. During the examination, the teacher notes the presence of gross visible defects in the structure of the articulatory apparatus (cleft lip, palate, short hyoid frenulum, abnormal dentition structure, malocclusion, such children need consultation with an orthodontist
Then he writes down the state of sound pronunciation in a notebook:
• Sound skipping
• Sound replacement
• Sound distortion (there is sound, but it doesn’t sound right)
• Sound mixing (in one case the sound is used correctly, in another it is replaced)
The state of the dictionary is also noted:
• Is the vocabulary age
• Does the child pronounce words correctly or distort them (abbreviates them, skips syllables, sounds; rearranges syllables, sounds; names only individual syllables).
Checking the state of phrasal speech , the teacher notes:
• How the child speaks – in phrases or only words;
• Does he construct the phrase correctly - does he coordinate the members of the sentence in gender, number, case, does he use prepositions in his speech, etc. ? d.
• state of coherent speech – can the child talk about an event, compose a story based on a picture, etc.
The teacher writes down in a notebook other features encountered in the child’s speech : loud, too fast, choking, slurred speech, etc. The examination allows the teacher to clearly present the general picture of the state of speech of children of the entire age group .
Speech development norms for children from 3 to 4 years old
Despite the fact that children of this age period may be at different levels of speech development, there are approximate guidelines that you can rely on when assessing your child’s speech. By the end of three years, the baby comes with the following achievements:
- His speech is clearer and his pronunciation has improved markedly.
- The baby can name almost all the objects around him: clothes, shoes, furniture, toys, interior items.
- More and more adjectives, adverbs, pronouns, and prepositions appear in speech.
- The child matches words by gender, case and number, but not always correctly.
- Children can remember and retell short poems and fairy tales.
Normally developing children of this age strive to communicate with peers and adults and actively establish contacts through speech.
How to determine delayed speech development in 3-year-old children
The development of a child’s speech at 3 years of age is most often accompanied by disturbances in motor skills and behavior. Specialists working with such children can say with full confidence that children with speech impairments exhibit the following signs of activity:
- Children are awkward, their movements are uncoordinated, they have poor balance;
- There is a noticeable lag in fine motor skills of the fingers, precise movements with small parts of toys and board games are inaccessible, children do not like to get dressed, fasten buttons, and cannot regulate the pressure on the pencil while drawing.
- Children are inattentive and constantly distracted;
- Among such children, manifestations of hyperactivity, or, conversely, inhibition are common.
The presence of these symptoms indicates that there are disorders of the central nervous system due to its organic failure. In some cases, delayed speech development (SDD) may be caused by unfavorable conditions for raising a child and his social environment.
Delayed speech development in 3-year-old children affects all aspects of speech: sound pronunciation, vocabulary, coherent speech, and its grammatical design. Possible problems:
- Children do not pronounce not only phrases, but also individual words; their speech remains at the level of babbling.
- There is no coordination of parts of speech; children's speech is similar to the speech of a foreigner who has just learned Russian. For example, “Tanya give me a kitty,” “Kolya went to bed,” “Mom sat down in a chair.”
- Whole groups of sounds are pronounced incorrectly, the child distorts or replaces some sounds with others, rearranges sounds and syllables not only in polysyllabic, but also in simple words. For example, nose - socks, eye - glasses, chamber - lapata.
- Prepositions are missing or used incorrectly (on, in, above, under, behind, before, between).
- The child's speech is unfluent, its pace is too fast or too slow.
- Phrases consist of 1–2, less often 3 words, they contain only nouns and verbs (“telegraphic” style of speech).
At this age, most children are already aware of the limitations of their speech capabilities. Since SRD prevents them from contacting peers and adults, these children may exhibit negativism, isolation, and increased irritability.
Speech therapy examination of a child of the first year of life
Violation of the prerequisites for speech formation in children of the 1st year of life is, as a rule, a consequence of damage to the central nervous system of various origins, as well as a consequence of a combination of various unfavorable factors: biological, social. Harmful factors affecting the brain during the period of its intensive development lead to developmental delays. However, examination of the pre-linguistic development of a child of the 1st year of life often presents great difficulties due to the physiological immaturity of the nervous system and the evolutionary and age-related characteristics of the developing brain.
Early identification of various deviations in speech formation will make it possible to begin correctional work in the 1st year of a child’s life and, thus, make it possible to compensate for the primary defect and prevent secondary deviations in speech development at a later age.
The proposed methodology is based on a comprehensive study of a child of the 1st year of life: the assessment of his pre-speech and pre-speech capabilities is carried out taking into account the characteristics of neuropsychic development and the characteristics of movement disorders. This is determined by the close relationship between the development of speech, motor skills, sensory functions and emotions, both under normal and pathological conditions. Therefore, a comprehensive examination is carried out on the basis of diagnosing the neuropsychic development of children in the 1st year of life.
A speech therapy examination includes the collection of data on early pre-speech development (analysis of extracts from the history of development, from the medical history, etc.), as well as data from observation and examination of the child.
A general examination must begin with observing the child while he is awake in a crib, playpen, etc., without attracting his attention to himself. This makes it possible to assess the position of the child’s body, his behavior, emotional and vocal reactions, and involuntary movements.
Then they pay attention to the shape of the baby’s skull as a whole and the ratio of the size of the brain and facial parts of the skull. In newborns, the shape of the skull can be very diverse, which is associated with its temporary deformation during the passage of the birth canal, but brachycephalic usually predominates. Head deformation associated with childbirth, after 2-3 weeks. disappears. Rarely does the skull have a tower shape. With hydrocephalus, the predominance of the cerebral part of the skull over the facial part is especially pronounced. With microcephaly, on the contrary, the size of the facial part of the skull predominates.
It is also necessary to note the presence of craniofacial asymmetries. Asymmetry of the bones of the brain and facial skull may be a constitutional feature, or may also be due to dysembryogenesis (Table).
Table. Basic dysembryogenetic stigmas
| Localization | Nature of the anomaly |
| Scull | The shape of the skull is microcephalic, hydrocephalic brachycephalic, dolichocephalic, brachycephalic, dolichocephalic, asymmetrical; low forehead, pronounced brow ridges, overhanging occipital bone, flattened occiput, hypoplasia of the mastoid processes. |
| Face | Straight line of sloping forehead and nose. Mongoloid and anti-Mongoloid eye shape. Hypo- and hypertelorism. Saddle nose, flattened nasal bridge, crooked nose. Facial asymmetry. Macrognathia, micrognathia, progenia, microgenia, cleft chin, wedge-shaped chin. |
| Eyes | Epicanthus, Indian fold of the eyelid, low standing eyelids, asymmetry of the palpebral fissures, absence of the lacrimal caruncle, enlargement of the lacrimal caruncle (third eyelid), distichnasis (double eyelash growth), coloboma, heterochromia of the iris, irregular shape of the pupils. |
| Ears | Large protruding ears, small deformed ears, ears of different sizes, different levels of ears, low-set ears. Anomaly in the development of the helix and antihelix, fused earlobes. Additional tragus. |
| Mouth | Microstomia, macrostomia, “carp mouth”, high narrow palate, high flattened palate, arched palate, short frenulum of the tongue, folded tongue, forked tongue. |
| Neck | Short, long, torticollis, pterygoid folds, excess folds. |
| Torso | Long, short, depressed breasts, chicken breasts, barrel-shaped, asymmetrical, large distance between the nipples, accessory nipples, agenesis of the xiphoid process, diastasis of the rectus abdominis muscles, low navel, hernia. |
| Brushes | Brachydactyly, arachnodactyly, syndactyly, transverse groove of the palm, flexion contracture of the fingers, short curved 5th finger, curvature of all fingers. |
| Feet | Brachydactyly, arachnodactyly, syndactyly, sandal cleft, bident, trident, cavus foot, overlapping toes. |
| Genitals | Cryptorchidism, phimosis, underdevelopment of the penis, underdevelopment of the labia, enlargement of the clitoris. |
| Leather | Depigmented and hyperpigmented spots, large birthmarks with hair, excessive local hair growth, hemangiomas, areas of aplasia of the scalp. |
The normal innervation of the facial muscles is evidenced by the symmetry of the palpebral fissures and folds on the face both in a calm state and during a cry, the symmetrical closure of the eyelids, and the tight grip of the nipple.
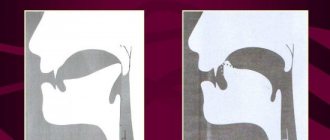
With paresis and paralysis of the facial muscles, a complex of symptoms is observed: widening of the palpebral fissure - lagophthalmos; when screaming, when a child tries to close his eyelids, the eyeballs move upward, but the palpebral fissure remains open and the white membrane under the iris is visible - Bell's phenomenon, one corner of the mouth may be lowered, one nasolabial fold may be more pronounced than the other. During screaming, uneven formation of folds on the forehead, pulling of the mouth to one side, loose grip of the pacifier, and leakage of food from the corner of the mouth are noted. All this may indicate peripheral damage to the facial nerve. With central damage to the facial nerve, lagophthalmos and Bell's phenomenon are absent, smoothness of the nasolabial fold is observed, and when screaming, the mouth is pulled towards a deeper fold. The tone of facial muscles, as well as the presence or absence of paresis and paralysis, is determined by a speech therapist during a joint examination of the child with a neurologist.
The study of the articulatory apparatus includes an assessment of the structural features of the articulatory organs, the resting position in the general symmetrical position of the child’s body, an assessment of involuntary movements of the articulatory apparatus during eating (sucking, swallowing, taking food from a spoon, drinking from a cup, biting, chewing, etc. ), with facial expressions, with vocal and sound reactions, as well as the presence or absence of paresis, paralysis, and violent movements. Muscle tone in the organs of articulation is determined during a joint examination by a speech therapist and a neurologist. By the way the child sucks and swallows and how these processes are combined with breathing, one can judge the function of the trigeminal, facial, sublingual (sucking), glossopharyngeal and vagus (swallowing) nerves.
With active sucking, the child sucks out the required amount of milk in 10-15 minutes, the milk does not pour out of the mouth, the child does not choke, the sucking is rhythmic and for every two sucking movements there are two swallowing movements and one or two breathing movements.
If the child does not grasp the nipple tightly, sucks sluggishly, gets tired, chokes, screams when sucking, holds milk in his mouth for a long time, and there is a nasal tone in the voice, this indicates bulbar or pseudobulbar disorders.
With bulbar syndrome, these symptoms are combined with the absence of palatine and pharyngeal reflexes, drooping soft palate, leakage of food through the nose, and salivation. During the neonatal period and the first months of life, salivation may not be expressed or expressed weakly; most often it appears by 4 months when the child is in an upright position in the arms of an adult. With bulbar symptoms, the child is on tube feeding. With pseudobulbar symptoms, the palatine and pharyngeal reflexes increase. An isolated lesion of the hypoglossal nerve does not significantly impair sucking and swallowing. By making a child scream, you can detect a deviation of the tip of the tongue towards the paretic muscle (damage to the hypoglossal nerve).
Limited mobility of articulatory muscles is the main manifestation of paresis or paralysis of these muscles. There may be insufficient lifting of the tip of the tongue upward in the oral cavity, lack of expression of the tip of the tongue, limited ability of the tongue to move downwards, backwards, etc. All this does not make it possible to form a variety of sounds in humming, babbling, and subsequently in speech.
Disorders of muscle tone in the articulatory muscles are characterized by its increase (hypertonicity), leading to spasticity of the articulatory muscles, when there is a constant increase in tone in the muscles of the tongue and lips. The tongue is tense, pushed back, its back is curved, raised upward, the tip of the tongue is not pronounced.
Increased tone in the orbicularis oris muscle leads to spastic tension of the lips and tight closure of the mouth. Involuntary movements with hypertonicity and spasticity of the articulatory muscles are limited, which will subsequently lead to a violation of voluntary motor skills. In a 3-6 month old child, a violation of the tone of the articulatory muscles can already be clearly stated. Until 3-4 months, physiological hypertonicity predominates in children.
Violations of the tone of the articulatory muscles can also manifest themselves in the form of hypotension. With hypotonia, the tongue is thin, spread out in the oral cavity, the lips are flaccid, cannot close tightly, food leaks from the corners of the mouth, and when chewing, food falls out of the mouth. In this case, nosalization of the sounds of humming, babbling, and screaming may be noted.
Violations of tone can manifest themselves in the form of dystonia (changing the nature of muscle tone). At rest, low muscle tone may be noted, and during sound reactions the tone increases sharply.
An assessment of the state of articulatory muscle tone should be carried out by a speech therapist together with a neurologist. Muscle tone in the articulatory and facial muscles is studied during passive movements of the organs of articulation. Passive movements of the lower jaw (passive opening and closing of the mouth) with the child’s body positioned symmetrically (child in the “on his back” position) make it possible to assess the tone of the muscles of the lower jaw and masticatory muscles. Passive movements of the child’s lips: opening - closing the lips, stretching the lips - bringing them into a “tube” - make it possible to assess the tone in the lip muscles, the orbicularis oris muscle. Passive movements of the tongue when pushing the tongue to the sides, backwards (pressing on the tip of the tongue and pushing it back), when grasping the tip of the tongue with two fingers and pulling it forward make it possible to assess the tone of the tongue muscles.
Together with a neurologist, a speech therapist evaluates unconditioned reflexes, the absence or presence of pathological reflexes of oral automatism when examining children with severe organic damage to the central nervous system, children with movement disorder syndrome, and cerebral palsy (CP).
The next stage of examination of a child of the 1st year of life is to assess his respiratory activity. Breathing disorders in children with various cerebral disorders are caused by insufficiency of central regulation of breathing, as well as pathology of motor function.
Breathing improves significantly after the birth of a child. In the first months of a child’s life, the abdominal type of breathing predominates, breathing is shallow and frequent. After 6 months the abdominal type of breathing is replaced by mixed breathing, breathing becomes deeper and less frequent. Children with cerebral pathology often experience disturbances in coordination between breathing, sucking, swallowing, as well as between breathing, phonation and articulation. Characteristic disturbances in the rhythm of breathing: when pronouncing sounds, breathing becomes more frequent, after pronouncing sounds a shallow convulsive breath is taken, active exhalation is disrupted. The severity of respiratory disorders corresponds to the severity of general motor damage.
Then the speech therapist, while observing the child, evaluates his vocal reactions associated with vital physiological functions. In addition to screaming, vocal reactions of a newborn and a child in the first months of life include coughing, sneezing, sounds when sucking, and yawning.
Various pathological conditions can make even these vocal reactions difficult or impossible.
Muscular weakness of the articulatory and respiratory muscles makes the child's cry weak and quiet. The cry can be shrill, painful, with a nasal tint in case of anomalies in the structure of the nasopharynx, bulbar or pseudobulbar disorders. Vocal responses may be poor or absent altogether due to central nervous system depression.
By 2 months in a healthy child, a cry occurs when communication with him ceases or when the position of his body changes, and not just as a reaction to hunger, discomfort, etc. At subsequent stages, the cry takes on the character of an active protest reaction: at 6-9 months. a healthy child can scream when strangers appear at 12 months. the child screams loudly in response to the fact that the toy was taken away. In children with cerebral pathology, genetic and chromosomal diseases, a cry for a long time does not acquire intonation, expressiveness, or has extremely limited significance in the development of communication between a child and an adult, or remains the only means of communication between a child and an adult throughout the entire 1st year of life (in cases severe pathology of the central nervous system).
The speech therapist evaluates the child’s first vocal unconditional reflex reactions by observation. It is recommended to monitor the child immediately after sleep, before feeding and after feeding, when falling asleep.
During a speech therapy examination, the child’s sound reactions are assessed by observation: hooting, humming, babbling. For a speech therapy examination, it is important not only the absence or presence of these sound reactions, but also their qualitative characteristics. An extensive system for identifying stimuli that are significant for a particular child makes it possible to outline ways to stimulate sound reactions.
The speech therapist must accurately establish the level of communication between the child and the adult: is it only the tactile-emotional level (which is very typical for children with severe cerebral pathology, chromosomal diseases), or emotional-speech, or a combination of tactile-emotional communication with emotional-speech, inherent children with perinatal pathology, premature children raised in an orphanage, or the level of objective-effective communication. Knowing the level of communication and significant stimuli makes it possible to choose the right direction in correctional work.
It should be taken into account that communication does not appear immediately with the birth of a child, but develops gradually. It can be confirmed that a child has communication when the following four signs are observed: looking into the eyes of an adult (18-20 days); response smile to the influence of an adult (1 month); proactive smiles and motor revival (3 months); the desire to prolong emotional contact with an adult.
As long as some of these signs are observed, the process of establishing communication occurs; when all four signs are present, communication is established. In the 1st year of life, the development of communication goes through three stages: newborn, emotional communication and, finally, “business” communication or objective-effective communication.
The shortest stage is the newborn stage; it covers the 1st month of life, when the baby is prepared for contact with other people.
The second stage of emotional communication covers approximately the 2-6th month of a child’s life.
The third stage of objective-effective communication begins in the second half of the child’s life. Communication becomes “businesslike”; it is included in the practical cooperation of the child with the adult.
The speech therapy examination ends with a speech therapist’s conclusion and recommendations for corrective work with the child.
Self-diagnosis of speech delay
The main method for diagnosing mental retardation at home is to observe your child’s speech. While observing your baby, you should note how developed his vocabulary is, how many words he uses. For this purpose, play situations are created where children are encouraged to name objects and toys, and small performances are performed with his toys. You need to carefully analyze how the baby constructs phrases and how many words they consist of.
To assess a child’s understanding of adult speech, you can offer him the following tasks:
- Show parts of your body, body parts of toy animals;
- Show in story pictures what their characters are doing. For example, who is running, who is watering the flowers, who is feeding the chickens, who is sleeping;
- Give simple instructions consisting of at least two steps. For example, first take a doll from the closet, and then put it on a chair;
- Ask about the purpose of the items. For example, show what you eat, wipe your hands, brush your teeth;
- Read a short text and ask questions about its content.
It is necessary to note what sounds the baby pronounces incorrectly, what sounds he replaces with those he pronounces. The child’s ability to retell a short fairy tale and his ability to use intonation are assessed. In addition to assessing speech, you need to pay attention to the state of general and fine motor skills. The following indicators are checked:
- Does the child maintain balance when walking and running?
- can he step over objects?
- how he catches the ball
- can he climb?
- does one maintain balance on a reduced area of support while standing on one leg,
- can he fasten buttons?
- Is the baby able to make precise movements with his fingers?
If the development of a child’s speech and motor skills deviates from the norm, you should consult a specialist and undergo the recommended in-depth examination. If there is a need for this, you need to start corrective work with a speech therapist, defectologist, or psychologist.