Forms of aphasia
In the first days after a cerebrovascular accident, speech disorders in patients may manifest themselves in the form of total aphasia
: the patient does not speak and does not understand speech addressed to him.
Total aphasia after a few days or weeks may be replaced by sensory
or
motor aphasia
: the patient begins to understand speech addressed to him, but communicates with others using a speech “embolus” - a stereotypically repeated sound combination, syllable or word, sometimes well intoned.
There are several forms of aphasia
However, two main
forms of aphasia
:
- sensory
- motor
Aphasia and speech: types
There are several classifications of aphasia. According to one of these classifications, aphasia is divided into the following clinical variants:
- Total - in this case, the victim absolutely does not understand the speech addressed to him and cannot address others. This form occurs in the first days after serious brain damage, for example, with extensive acute cerebrovascular accident.
Sensory or motor aphasia - occurs in a more distant period after damage to the nervous tissue of the brain. The patient is aware of the speech addressed to him, but at the same time, his own speech forms a so-called “speech embolus” - a repeatedly repeated sound combination or words pronounced with different intonation.
- Wernicke's sensory aphasia is a form of aphasia in which speech understanding is impaired, while the ability to speak is preserved. The patient talks a lot continuously, however, he himself does not realize the meaning of what was said.
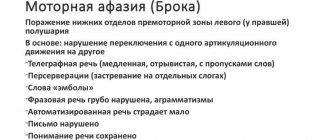
- Broca's motor aphasia is characterized by a violation of the ability to speak while maintaining the understanding of speech, both that of others and one's own.
The most popular classification in the Russian Federation is the classification of A.R. Luria, who identifies the following types of aphasia:
- Dynamic – characterized by a defect in internal speech and the inability to formulate, express and implement it. It occurs as a result of trauma to the prefrontal region of the left hemisphere.
- Afferent motor aphasia - manifests itself when the parietal and posterior-central region of cortical structures are damaged. The key defect is the inability to correctly select the right sound for the correct pronunciation of a word. Those. the patient is unable to distinguish sounds that are similar in pronunciation.
- Efferent motor aphasia or Broca's aphasia. It manifests itself in a “telegraphic” style of speaking and problems switching from one word to another, as well as difficulties in reading and writing. Occurs due to injury to the lower parts of the cerebral cortex - the so-called Broca's speech motor center.
- Wernicke's aphasia or sensory aphasia is the loss of the ability to perceive the sound side of speech. Amnestic aphasia is manifested by difficulties in determining the name of an object, despite the fact that the patient knows what this object is for and how to use it. Occurs due to trauma to the parietotemporal region. Amnestic aphasia is divided into three forms: acoustic-mnestic, optical-mnestic and nominal. The acoustic-mnestic form is characterized by problems remembering incoming information, memory capacity is significantly reduced and auditory-speech perception is inhibited. In optical-mnestic aphasia, visual memory is affected. Nominal aphasia also involves difficulty naming objects and is also a symptom of Alzheimer's disease.
- Semantic aphasia - the main defect of this form of aphasia is manifested in a violation of the analysis of speech structures and speech synthesis.
According to foreign literature, another classification stands out:
- Non-fluent aphasia is manifested by difficulty pronouncing sentences and occurs when the anterior lobes of the cerebral hemispheres are traumatized.
- “Posterior” aphasia is characterized by the preservation of smooth and understandable speech. Occurs when the posterior parts of the hemispheres are damaged.
Sensory aphasia
Wernicke's sensory aphasia
is a violation of the understanding of speech, both someone else’s and one’s own, while maintaining the ability to speak.
Occurs when the left temporal lobe of the brain is damaged. As a rule, the patient speaks quite willingly and a lot, but due to the loss of understanding of what he hears, he does not understand either himself or those around him. The form of sensory aphasia
is characterized by two main features:
- the patient’s speech is incomprehensible to others due to the lack of meaning in it (misunderstanding of one’s own speech leads to loss of control over it, the patient invents new words, replaces letters or syllables in existing ones, swaps words, pronounces incoherent strings of words and sentences)
- the speech of others and his own is incomprehensible to the patient (due to impaired perception of sound, loss of distinction in the sound composition of words, the patient does not understand the meaning of what he hears)
RESTORATION OF SPEECH IN PATIENTS WITH APHASIA AT THE EARLY STAGE AFTER STROKE
A stroke (synonymous with acute cerebrovascular accident) is the death of a part of the brain associated with the cessation of its blood supply. Impaired blood supply to certain areas of the brain leads to the appearance of aphasia. Aphasia comes in various forms and degrees of severity - from minor difficulties in articulating or naming objects to complete loss of understanding speech or verbal expression of thoughts. In the first days after a cerebrovascular accident, speech disorders in patients manifest themselves in the form of total aphasia: the patient does not speak and does not understand speech addressed to him. With total aphasia, the patient cannot understand written and spoken speech. Usually the lesion is localized in the left hemisphere and is quite extensive.
If total aphasia is caused by vascular origin, then patients often experience a tendency to slow speech recovery. In this case, the type of speech disorders may be similar to Broca's aphasia, or some other types of this disease. Typically, total aphasia occurs as a result of a stroke, when the sensory and motor parts of speech are simultaneously affected. This process involves the entire region of the cerebral middle artery. Total aphasia after a few days or weeks can be replaced by gross motor aphasia: the patient begins to understand speech addressed to him, but communicates with others using a speech “embolus” - a stereotypically repeated sound combination, syllable or word, sometimes well intoned.
Speech therapy classes for total aphasia begin with the restoration of listening comprehension. The method of stimulating the understanding of speech by ear for patients with total aphasia is based on their correlating intonations with gestures, inducing certain motor and facial reactions in the patient, and using the phonological features of intonations. To stimulate listening comprehension of speech, a patient with total aphasia is asked to perform various actions according to oral instructions.
Restorative learning is based on one of the most important properties of the brain - the ability to compensate. To restore impaired functions, both direct and bypass compensatory mechanisms are used.
The first is associated with the use of direct disinhibiting methods of work. They are mainly used in the initial stage of the disease and are designed to use reserve intrafunctional capabilities. Techniques and methods of disinhibition during the learning process come down mainly to various activation of speech activity and the removal of inhibitory background. Patients are persistently stimulated through various tasks for active verbal communication. The following techniques and exercises are used:
- Ordinal counting from 1 to 10.
— Count from any arbitrary number (from 5, 6, etc.).
— Highlight any number (or two). We count from 1 to 10, but when
In this case, we pronounce the highlighted numbers loudly, the rest - in a whisper (in an undertone).
- The same techniques, only the counting occurs in reverse order.
- Naming the days of the week.
- Listing the months of the year.
Bypass methods involve voluntary mastery of the way of perceiving speech and one's own speaking. This is due to the fact that bypass methods require the patient to implement the affected function in a new way, which differs from the usual one established in premorbid speech practice. Restoring a number of speech functions requires the connection of non-speech supports. Therefore, the sequence of work on speech and non-speech functions is decided in each specific case, depending on the combination of verbal and non-verbal components of the syndrome. Bypass methods imply compensation based on the restructuring of the most impaired function due to cross-functional restructuring. In other words, the restorative effect is achieved through the introduction of new, “workaround” ways of performing certain speech or gnostic-praxic operations. Speech restoration is facilitated by:
- involving the patient in simple non-speech activities, for example:
- constructing cubes, putting together puzzles, sketching, drawing objects, plots, etc.
— game of lotto, dominoes, playing cards.
— laying out serial pictures, plots.
- using tasks that require speech understanding:
- showing body parts,
- showing objects, actions in pictures,
- following simple instructions.
- stimulating simple dialogues that require a response in one or two words or a gesture.
- Encouraging reading and writing by offering activities such as:
- placing captions under pictures,
- work with subject lotto,
- naming (or choosing from the proposed) numbers, letters,
- recording from dictation (or choosing from the suggested) numbers, letters,
- writing and reading familiar and simple words and phrases.
Rehabilitation training is carried out according to a special, pre-developed program. The program should include certain tasks and corresponding work methods, differentiated depending on the form of aphasia, the severity of the defect, the stage of the disease, and the individual characteristics of speech disorders. After conducting a speech therapy examination of a patient with total aphasia, we developed an individual plan for speech therapy work.
Patient E. 72 years old. Acute cerebrovascular accident of the left middle cerebral artery on March 31, 2014.
Neuropsychological speech therapy examination.
He makes no complaints due to the complexity of his speech disorder.
Objectively:
- Impressive speech: understands situational and everyday speech, understanding complex lexical and grammatical constructions is difficult. The latency period for completing tasks has been increased.
Expressive speech: represented by “embolus” (dvvvu).
Phonemic hearing is impaired.
Oral articulatory praxis is impaired.
Reading and writing are in decline.
Nominations are shown based on pictures selectively.
Automated, de-automated speech is impaired.
- Shape and position of the tongue in the midline. No deviations were found.
Swallowing is not impaired.
Subtle differentiated movements of the tongue and sound pronunciation could not be studied.
The tone of the tongue muscles is increased.
Conclusion: efferent-afferent motor aphasia. Sensory aphasia. Speech impairment of the first degree of severity.
Work plan:
- Restoring understanding of spoken speech: captioning pictures; cheating; decomposition of pictures.
- Overcoming oral-articulatory apraxia, working with automated rows (disinhibition)
- Non-verbal activities (solving examples, dominoes, lotto, classifications, eliminating the odd one out).
Thus, speech restoration in severe forms of aphasia includes both stimulation of listening comprehension and disinhibition of the expressive side of speech.
Speech therapy work for aphasia is a long and labor-intensive process that requires the cooperation of the doctor, speech therapist, patient and his immediate environment, and speech restoration should not take place empirically, but skillfully, at a serious professional level. Therefore, it is important to select patients for intensive rehabilitation treatment and training. The prognostic significance of individual factors affecting the effectiveness of recovery (age, premorbid level, motivation, signs of left-handedness, somatic diseases and their dynamics) should be taken into account.
List of used literature:
- Rustle - Trotskaya, M.K. Strategies and tactics for speech restoration. / M.K. Rustle - Trotskaya. – M.: EKSMO Press, V. Sekachev, 2001. – 432 p.
- Shklovsky, V.M., Wiesel, T.G. Restoration of speech function in patients with different forms of aphasia, M.: “Association of Defectologists”, V. Sekachev, 2000. - 96 p.
- Wiesel, T.G. Neuropsychological blitz examination - M.: V. Sekachev, 2005.-24 p.
Motor aphasia
Broca's motor aphasia
is a violation of the ability to speak while maintaining the ability to understand speech. Occurs when the frontal lobe of the brain (Broca's motor speech center) is damaged. The patient has difficulty pronouncing or does not pronounce words, mainly pronouncing simple words or syllables. The main features of the form of motor aphasia are:
- the patient’s speech is poorly distinguishable, but is often understandable and meaningful, accompanied by eloquent gestures (the patient has difficulty pronouncing and moving from one word to another)
- the speech of others is well understood by the patient
Definition of aphasia
Literally, the term aphasia is translated from Greek as “I don’t speak.” As a rule, this pathology occurs in the adult population, but it is quite possible for it to develop in children whose speech has more or less developed, that is, from three years of age and older.
In clinical neurological practice, the term aphasia has the following meaning: it is a disorder of speech function of a systemic nature, consisting of either partial or total loss of formed speech function. This definition implies the presence of a defect in the central nervous system, the presence of damage to the speech zones of the cerebral cortex and the resulting speech disorders that affect both internal and external speech.
Clinically, aphasia can have varying degrees of severity and, as a rule, is not the only or isolated manifestation of brain damage. Moreover, its development and severity depend on the location and volume of the lesion.
Treatment of aphasia
Treatment of aphasia
in most cases it is successful. There are special speech restoration programs for different forms of aphasia, which are differentiated. In the process of individual work with patients with aphasia, a speech therapist modifies the techniques and methods of correctional pedagogical work available in the arsenal of defectology, bringing his own individual experience.
Treatment of aphasia
consists not only in restoring ability, but also in restoring the affected part of the brain, which is the cause of the speech disorder.
If you or your loved ones have speech problems, make an appointment with a speech therapist. At the “Your Health” clinic, appointments are conducted by a highly qualified specialist with many years of experience in the specialty “Speech Therapy” Ella Borisovna Rothbert, who will help you choose the optimal method of speech correction.
There are several forms of aphasia, which are characterized by a violation of either speech understanding or speech reproduction. In severe cases of aphasia, a person’s ability to both understand others and speak is impaired. This speech disorder most often occurs in older people as a consequence of severe brain diseases (stroke, tumors) or brain injuries.
In children, aphasia is diagnosed when organic brain damage occurs after the child has mastered speech. In this case, aphasia leads to disruption of its further development, sometimes to the collapse of formed speech. Aphasia often leads to profound disability.
The possibilities for compensation for speech and mental disorders in children and adults are sharply limited. Adults with aphasia, as a rule, lose their profession and have difficulty adapting to everyday life. Misunderstanding of others and the inability to express one’s desires cause behavioral disorders: aggression, conflict, irritability.
Finally, the last fundamental point that we have laid as the basis for speech rehabilitation work is the principle of selecting words according to their emotional and semantic significance for the patient, and not according to the principle of phonemic “ease” for pronunciation.
What can a patient with aphasia say? Everyone knows that often a patient who cannot voluntarily pronounce a single word retains “speech emboli”, which are quite complex in their phonemic composition. This means that the patient (except for isolated cases of aphasia, which is based on severe apraxia of the speech organs) can pronounce very complex phonemic combinations. With severe apraxia of the speech organs, the patient will not have a speech embolus; he is simply silent or makes unarticulated sounds. Sometimes a single syllable becomes an “embolus”. However, in that form of aphasia, which is characterized by the presence of verbal or phraseological “speech emboli,” only their trigger and mechanism is disinhibited, while the rest of the speech system, for some reason, turns out to be inhibited. This means that the task is to disinhibit the speech system, slowing down the “embolus”, which often, if not treated attentively, turns into a “trigger mechanism” for any utterance.
The generally accepted point of view that labial consonants are “easier” to pronounce in the first stages of rehabilitation work than front-lingual consonants is also not justified in practice. On the contrary, it seems that the front-lingual ones are more often preserved in aphasia than the labial ones. In any case, for many patients in the first stages of rehabilitation work, pronunciation of front-lingual words is easier than labial ones.
However, this does not mean that some patients should be given words that include some anterior lingual sounds, while others should be given words with labial consonants. We often see patients who, being unable to pronounce this or that phoneme in a word that has no semantic-emotional significance for them, easily pronounce it in a word that is meaningful to them. So, for example, patient R., 56 years old (in the initial period - total aphasia after a repeated stroke), was completely unable to voluntarily raise her tongue to the upper teeth and did not pronounce back-lingual words in most words, but at the same time she clearly pronounces “k” in the words “so” (if she is satisfied with the way she repeated the word) and “flour” if she failed to repeat the word. Or patient G., 47 years old, who for a long time could not pronounce (find articulation) the sound “f”, immediately found its pronunciation in the words “fermato” or “forte” (the patient is a pianist by profession).
Treatment methods
The form and cause of aphasia determines treatment tactics. Initially, they try to influence the cause of the disease, for example, oncology, inflammation, changes in cerebral circulation. You need to understand that with aphasia, speech restoration takes a long period and requires a competent approach. Complex therapy includes both medication, physiotherapeutic treatment, and speech therapy. Only under these conditions is it possible to provide high-quality correction of the patient’s speech disorders.