What is dynamic aphasia?
Dynamic aphasia is a local absence or disturbance of already formed speech due to the inability to form internal speech and express it. Most often it occurs as a result of damage to the prefrontal region of the left hemisphere in right-handed people and vice versa, that is, the departments of the third functional block - activation, regulation and planning of speech function.
Dynamic aphasia syndrome was first discovered in the middle of the last century in 1934 by physician and researcher Karl Kleist. He put forward the hypothesis that with this type of aphasia there is a violation of the formation of spontaneous speech. Later, A.R. became interested in this topic. Luria, who in turn suggested that despite the impairment of developed spontaneous speech, the motor and sensory components are preserved in the victim.
The dynamic form of aphasia is characterized by a violation of the formation of written and oral active speech; difficulties arise in perceiving some information and performing certain thought processes. At the same time, patients with such forms of aphasia are not able to independently construct a sentence and have difficulty in correctly constructing words, which leads to a large number of grammatical errors. It is difficult for such people to perceive verbs and carry out any commands and actions.
Acoustic-mnestic aphasia
Cause
acoustic-mnestic aphasia - damage to the middle and posterior parts of the temporal region.
It is characterized by symptoms such as a decrease in auditory-verbal memory
due to inhibition of auditory control. When listening to each new word, the patient loses understanding of the previous one, hence the repeated repetition of the same syllable or word. An aphasic who suffers from the acoustic-mnestic form cannot repeat 3-4 words in a row with different meanings. For example, sky, hand, grass, spoon, repeats either the first or the last word. Phonemic hearing and correct articulation are preserved, which results in verbosity that compensates for communication difficulties. The nominative function of speech, retelling based on plot pictures, suffers. Misunderstanding of the meaning of words leads to verbal paraphasia - substitution of words in a sentence, merging one word into one in writing. Along with writing, counting and reading are impaired.
Up
Speech apparatus device
The functioning of the nervous system of the human brain is designed in such a way that we do not have to think every second about every action we take. Most parts of the central nervous system operate autonomously, i.e. independent mode and all this thanks to millions of electrochemical connections both between individual neurons and between higher nerve centers. The speech apparatus of an adult consists of several centers and is a complex structure that, thanks to nerve connections, functions as a single whole. The main role in the development and activation of speech function is played by the brain speech and analytical centers of Wernicke and Broca.
Causes of dynamic aphasia
The formation of the pathological process is based on a disruption in the functioning of cortical structures in the region of the speech center of the brain. In the case of dynamic aphasia, patients suffer damage to the posterior frontal parts of the left hemisphere - in a place located in close proximity to Broca's area. This fact influences the characteristics of the manifestation of this form of aphasia - a decrease in spoken speech. The patient’s speech becomes “poor”, verbs are missing or skipped, and the patient requires stimulating questions.
There are quite a large number of risk factors, the main ones of which include:
- Complicated family history;
- Elderly and senile age;
- Vascular diseases including atherosclerosis;
- Arterial hypertension;
- Rheumatic heart diseases;
- Mechanical injuries and surgical interventions on the brain.
Among the causes of aphasia, the primacy is occupied by vascular diseases of the brain - discirculatory encephalopathies, acute cerebrovascular accidents. In addition, aphasia is caused by inflammatory diseases (meningo-encephalitis, brain abscess), diseases of the central nervous system of a chronic course - Pick's disease, Alzheimer's disease, oncogenic diseases of a benign and malignant nature, traumatic brain injuries.
Impressive speech
Sensory or impressive speech - understanding and perception of speech. In the cerebral cortex in the temporal gyrus there is an area (Wernicke's area) that is responsible for the perception of sensory speech.
In this zone, the assimilation and accumulation of all previously acquired words and their sound images occurs. When this zone is damaged, a person hears words, but ceases to understand their meaning. With normal hearing intact, the patient does not perceive words addressed to him, since they are meaningless to him.
Classification
Currently, there are a large number of different classifications of aphasia. In the Russian Federation, the classification most often used is A.R. Luria, which reflects all clinical types of aphasia:
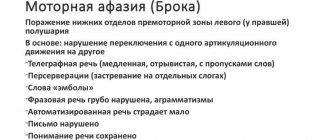
- Efferent motor aphasia, this form occurs in case of damage to the lower parts of the cortex - Broca's center. It is characterized by the collapse of grammatical structures into sentences and the difficulty of restructuring from one word to another. Serious reading and writing impairments occur.
- Afferent motor aphasia. Occurs when an area of the parietal cortex or posterior area is affected. The key disorder in this aphasia is the inability to detect the necessary articulatory position of the lips, tongue and speech facial muscles for the correct pronunciation of a word.
- Dynamic aphasia - occurs when the prefrontal or perifrontal part of the cerebral cortex is damaged. It is manifested by the lack of possibility of adequate construction of internal speech and its implementation aurally.
- Semantic aphasia - it is based on a defect in understanding complex speech structures and simultaneous analysis of information.
Diagnosis and treatment methods for aphasia in Moscow
The problem can be resolved with the help of qualified specialists. The disease requires elimination of the main cause and further correction. The speed of its correction largely depends on the degree of brain damage, so it is important not to delay a visit to a specialist. Diagnosis and treatment of speech disorders is carried out by specialists from the Department of Neurology.
At the initial appointment, the doctor collects anamnesis, collects complaints (in the case of aphasia, if it is impossible to independently describe the condition, close relatives are involved in the diagnosis), conducts a general examination for the presence of external abnormalities (in particular, drooping corners of the lips, decreased tone of the limbs).
Additionally, an examination by a neurologist in a team with a speech pathologist-speech pathologist is required so that the nature of the disorder can be assessed and appropriate corrective measures can be selected. Initiation of therapy requires testing, including assessment of the following symptoms:
- Spontaneous speech. Speech is assessed by the number of words spoken, the presence of spontaneous errors, and the frequency of pauses to select suitable words.
- Understanding. The patient is asked to point to objects that the specialist names and answer basic questions (“yes” or “no”).
- Enumeration of objects. The patient is asked to say the name of the specific object that the specialist points to.
- Reading and writing. The patient is given the task of writing any phrase and saying it out loud. This allows you to assess the degree of understanding and pronunciation.
- Semantic activity. The doctor demands to name all the animals that the patient remembers in one minute.
Specialists
Aphasia is a neurological disease, which means that this pathology is treated by a specialist - a neurologist. Aphasia is treated either in multidisciplinary municipal hospitals in neurological departments, or in specialized centers. One of the most progressive and largest neurological centers is the Clinical Brain Institute. The clinic has a polyclinic, day and 24-hour hospitals that provide prevention, treatment and rehabilitation of patients with a wide variety of neurological pathologies. A speech restoration center operates on the basis of the rehabilitation block. It is in this center that patients who have suffered traumatic brain injuries, acute cerebrovascular accident and suffering from various forms of aphasia undergo treatment and correction.
In addition to the neurologist, a rehabilitation specialist, psychotherapist and speech therapist must take part in the treatment of patients with aphasia.
Diagnostics
Aphasia should be distinguished from alalia, in which the speech function is not initially formed. With aphasia, the loss of speech function is disrupted after its formation in childhood. This is why this diagnosis can be confidently made only in children who have reached three years of age or older. As a rule, aphasia is combined and affects various forms of speech activity, which requires a detailed study of the symptoms of each individual patient. Dynamic aphasia can be established as a result of composing a story based on a specific plot device or a series of sequential pictures. Retelling certain text passages or writing an essay on a specific topic can also help in establishing a clinical diagnosis.
In order to determine the cause of aphasia and the exact localization of the area of damage to the speech center, the specialist must prescribe one of the following studies:
- Tomographic studies – computer or magnetic resonance imaging of the brain;
- Ultrasound Doppler mapping of blood vessels in the brain, head and neck;
- Magnetic resonance angiography;
- Lumbar puncture.
Diagnostics and establishment of a clinical diagnosis of dynamic aphasia are carried out by specialists in related fields, namely: a neurologist, a neurosurgeon, a speech therapist, a psychotherapist.
MOTOR APHASIA OF AFFERENT TYPE
Stage of severe disorders
1. Overcoming disorders of understanding situational and everyday speech:
- display of pictures and real images of the most commonly used objects and simple actions by their names, categorical and other characteristics. For example: “Show a table, a cup, a dog, etc.”, “Show pieces of furniture, clothing, transport, etc.” “Show someone who flies, who talks, who sings, who has a tail, etc.”
— classification of words by topic (for example: “Clothing”, “Furniture”, etc.) based on a subject picture;
— answers with an affirmative or negative gesture to simple situational questions. For example, “Is it winter now, summer..?”; "You live in Moscow?" and etc.
2. Disinhibition of the pronunciation side of speech:
- conjugate, reflected and independent pronunciation of automated speech series (ordinal counting, days of the week, months in order, singing with words, ending proverbs and phrases with a “hard” context), modeling situations that stimulate the pronunciation of onomatopoeic pronouns (“ah!” “oh” !" and so on.);
- conjugate and reflected pronunciation of simple words and phrases;
- inhibition of the speech embolus by introducing it into a word (ta, ta..-Tata, so), or into a phrase (ma..ma-mama...; this is mom).
3. Stimulating simple communicative types of speech:
— answers to questions in one or two words in a simple situational dialogue;
— modeling situations that contribute to the evocation of communicatively significant words (yes, no, want, will, etc.);
— answers to situational questions and composing simple phrases using a pictogram and a gesture accompanied by the pronunciation of simple words and phrases.
4. Stimulating global reading and writing:
— laying out captions under pictures (subject and subject);
- writing the most common words-ideograms, copying simple texts;
— conjugate reading of simple dialogues.
Moderate stage of disorders
1. Overcoming disorders of the pronunciation side of speech:
- isolating sounds from words;
— automation of individual articles in words with different syllabic structures;
— overcoming literal paraphasias by selecting first discrete and then gradually converging sounds in articulation.
2. Restoration and correction of phrasal speech:
- composing phrases based on a plot picture: from simple models (subject-predicate, subject-predicate-object) to more complex ones, including objects with prepositions, negative words, etc.;
- composing phrases on questions, on key words;
- exteriorization of grammatical-semantic connections of the predicate: “who?”, “why?”, “when?”, “where?” etc.;
— filling in gaps in a phrase with a grammatical change in a word;
— detailed answers to questions;
- compiling stories based on a series of plot pictures;
- retelling texts based on questions.
3. Work on the semantics of the word:
— development of generalized concepts;
- semantic play on words (subject and verbal vocabulary) by including them in various semantic contexts;
— filling in the gaps in a phrase;
- completing sentences with different words that are appropriate in meaning;
- selection of antonyms, synonyms.
4. Restoration of analytical-synthetic writing and reading:
- the sound-letter composition of the word, its analysis (one-two-three-syllable words) based on diagrams that convey the syllabic and sound-letter structure of the word, a gradual reduction in the number of external supports;
- filling in missing letters and syllables in words;
- copying words, phrases and small texts with an emphasis on self-control and independent error correction;>
- reading and writing from dictation of words with a gradually more complex sound structure, simple phrases, as well as individual syllables and letters;
- filling in missing words in texts when reading and writing, practiced in oral speech.
Stage of mild disorders
1. Further correction of the pronunciation aspect of speech:
— clarification with articles of individual sounds, especially affricates and diphthongs;
— differentiation of acoustic and kinesthetic images that are similar in articulation of sounds in order to eliminate literal paraphasias;
- practicing the purity of pronunciation of individual sounds in a sound stream, in phrases, with a combination of consonant sounds, in tongue twisters, etc.
2. Formation of detailed speech, complicated in semantic and syntactic structure:
- filling in the missing main sentence, as well as a subordinate sentence or subordinating conjunction in a complex sentence;
- answering questions with complex sentences;
- retelling texts without relying on questions;
— drawing up detailed plans for texts;
— preparation of thematic messages (short reports);
- speech improvisations on a given topic.
3. Further work to restore the semantic structure of the word:
- interpretation of individual words, mainly with abstract meaning;
— explanation of homonyms, metaphors, proverbs, phraseological units.
4. Work on understanding complex logical and grammatical figures of speech:
— execution of instructions, including logical and grammatical phrases;
— introduction of additional words, pictures, questions that facilitate the perception of complex speech structures.
5. Further restoration of reading and writing:
- reading and retelling expanded texts;
- dictations;
— written presentation of texts;
— writing letters, greeting cards, etc.;
- essays on a given topic.
1) Restoring the “articuleme-phoneme” connection
- writing letters corresponding to the names of sounds in expressive speech, reading these letters immediately after writing;
- isolating the first sound from simple words, fixing attention on the articulatory, acoustic, and then graphic image of this sound; independent selection of words for this sound and writing them;
- writing practiced sounds and syllables under dictation;
— identification of letters in different fonts;
— finding given letters in various texts (underlining, writing out).
2) Restoring the ability to sound-letter analysis of the composition of a word:
- dividing words into syllables, syllables into letters (sounds) based on various graphic schemes;
- highlighting any sound in a word;
- recalculation and listing of words by letter (orally);
- filling in gaps in words;
- writing words from letters given separately.
3) Restoring the skill of detailed written speech:
- writing words of different sound structures with and without support from an object picture: a) under dictation, b) when naming an object or action;
- writing proposals: a) from memory, b) from dictation, c) in the form of a written statement based on a plot picture for the purpose of communication with others;
- written statements and essays.
Treatment
First of all, you need to cure the underlying disease that caused the development of aphasia. To correct emerging symptoms, an integrated approach is used, including drug therapy, physiotherapeutic treatment, active rehabilitation, speech correction together with a speech therapist, as well as neuropsychological correction. Rehabilitation therapy should begin as early as possible, from the first days or weeks after the incident, as soon as the patient’s general condition allows. This is necessary to prevent the consolidation of pathological speech symptoms, the main of which are:
- Paraphasia is a speech disorder in which the logical structure of a sentence is disrupted and its semantic load is lost;
- Agrammatism is a difficulty in understanding sentences, especially those with complex syntax. Agrammatism occurs with a pathological focus localized in the Sylvian fissure;
At each stage of rehabilitation therapy, the joint work of the attending physician, psychologist, speech therapist, and especially the patient’s relatives is necessary. Only constant contact and communication will help achieve maximum effectiveness of treatment and rehabilitation procedures, as well as stabilize the patient’s general condition and mood. The speed of recovery processes and the mood in line with the patient’s wishes depend on how often and how much close and relatives communicate with the victim.
Drug therapy
Treatment of the underlying disease is carried out under the supervision of a neurologist or neurosurgeon. Drug therapy includes the following classes of drugs:
- Antioxidants and vitamins. These drugs are necessary to maintain a sufficiently active metabolic function of neurocytes. Antioxidants help accelerate regenerative and repair processes at the ultracellular level, stabilize cell membranes and protect them from lipid peroxidation. Among vitamins, a special role is played by B vitamins, which have a pronounced neuroprotective effect. B vitamins include: pyridoxine, pyrimidine, thiamine, folic acid, cyanocobalamin, riboflavin. Complex preparations of vitamins and antioxidants effective for dynamic aphasia include: Mexidol, Glycine (Lipoic acid), Aspirin, Emoxipin.
- Nootropic drugs. This group of drugs improves cerebral circulation and has a positive effect on metabolism in brain tissue. Nootropics have an antihypoxic and tranquilizing effect without inhibiting the activity of the central nervous system, which makes their use safe for everyday independent use. Taking nootropics is not accompanied by drowsiness, lethargy and relaxation of skeletal muscles. In addition, the drugs have a psychostimulating effect, restore mental performance and physical activity. This group of drugs includes all racetam derivatives (Piracetam, Nootropil), Picamelon, Cerebrolysin.
- Cerebroprotectors. Prescribed to prevent the development of complications and irreversible damage to neurocytes as a result of metabolic disorders or hypoxic shock, it affects metabolism, thereby improving blood supply to the brain. The main representatives are Vinpocetine, Cinnarizine, Coplamin.
- Vasoactive drugs - improve cerebral blood supply. This includes several different groups of drugs: antiplatelet agents (Clopidogrel, Plavix), anticoagulants (Sincumar, Warfarin, Heparin), calcium channel blockers (Nimodipine), methylxanthines (Pentoxtrental).
Speech therapy correction
The choice of a correctional work program primarily depends on the volume of the affected area of the brain and the severity of the clinical manifestations of dynamic aphasia. At the very beginning of rehabilitation, a restoration process is carried out, which begins with passive work with the patient, while methods are used to promote speech disinhibition and prevent the development of further speech disorders. Subsequently, the speech therapist draws up an individual plan and selects individual exercises for a particular patient. The duration of speech therapy correction for disorders associated with the development of aphasia averages about two to three years. The work uses special techniques for constructing sentences that allow the patient to reconstruct a detailed statement on his own. Work is also underway to correct the communicative function and self-control over it. Only when the patient understands the nature of his grammatical errors can one create opportunities for him to independently control his speech, the course of the narrative, and correct paraphasias.
The main emphasis of speech therapy work for dynamic aphasia is the elimination of defects in internal planning and programming of speech, as well as stimulation of speech activity.
Neuropsychic correction
Neuropsychological correction of speech in dynamic aphasia, regardless of the form of aphasia, deals with correction of all aspects of speech, namely its understanding, reproduction, writing and reading. The goal of neuropedagogical speech restoration for aphasia is to generally disinhibit speech, reduce the number of errors, improve the patient’s mental state and his interest in communication, as well as activity in general. The program plan is developed taking into account the individual characteristics of the lesion and the severity of the pathology. For this purpose, specific techniques are used, such as:
- “Having completed the mind” - the poem is read to the patient several times, after which the specialist begins the sentence, and the patient finishes it;
- Verbalization of one’s own actions - the patient is asked to talk about the progress of his day using drawing, reading and writing;
- Rhythmic-myological exercises – the patient learns light rhythmic songs, tongue twisters;
- Techniques of conjugate and reflected repetition;
- Semantic selection of words.
Physiotherapeutic treatment
Physiotherapy is prescribed in cases of traumatic brain injury, stroke and neurosurgery. The majority of patients are prescribed neuromyostimulation, which helps restore and strengthen the tone and strength of the facial muscles. Thanks to this method, myocytes are stimulated due to electric current pulses, which makes it possible to restore the lost motor function of the facial muscles.
Patients are also recommended to engage in physical therapy according to an individually drawn up plan together with a personal approach to each person. After physical therapy exercises, tissue metabolism and a wide variety of metabolic processes are activated in the body and cerebral blood flow increases. At the same time, the patient becomes more active and his mood improves.
Another significant means of physiotherapeutic treatment is therapeutic massage. Massage has a tonic, relaxing, antispasmodic effect, activates the excitability of the nervous system, and increases muscle performance.
He understands everything, but cannot say
The main characteristic of dynamic aphasia is the inability to speak.
A person understands what is said, pronounces sounds correctly, repeats what others say, but cannot construct his own presentation of thoughts. With this disease, the regulatory function of speech is impaired - the patient is not able to construct a phrase plan and conduct an internal monologue, hence the impossibility of speaking. Therefore, the patient tries not to start a dialogue with strangers first: he is unable to construct a question or ask for something, and he is aware of this. Speech grammar is impaired, patients avoid verbs, prepositions and pronouns are omitted. Nouns are often used only in the nominative case.
Analysis of addressed speech in dynamic aphasia shows that reading and counting are not impaired, but when reading aloud, people with this disease may miss words and phrases and are unable to explain the meaning of the text. The ability to communicate through writing is retained in most cases, but only in simple phrases. Difficulties begin if you need to compose something yourself or write a complex grammatical structure from dictation.
Patients almost always lose the ability to maintain concentration on something for a long time and often become irritable or, conversely, indifferent because of this.
Prevention and prognosis for patients
Restoring the victim’s speech depends on a whole range of factors, the most important of which are:
- Localization and volume of affected brain tissue;
- Level of speech disorder;
- Time from the start of rehabilitation after injury or vascular lesion;
- The age of the victim and his general condition.
The best results are expected to be observed in younger people, however, do not be discouraged, since the reactivity of compensatory-restorative reserves is developed differently in each person and with intensive rehabilitation it can be significantly activated.
Prevention mainly consists of preventing the occurrence of repeated or recurrent episodes of the disease that provokes the development of aphasia. For this purpose, it is necessary to undergo timely and regular diagnostic examinations and correct even minor deviations from the norm. Patients who have already encountered clinically pronounced forms of aphasia and have undergone rehabilitation should still be periodically observed by neurologists or neurosurgeons.