Methods and techniques for working with dysarthrics.
“Basic methods and techniques of correctional work
with dysarthric children"
PLAN:
- Brief description of the characteristics of dysarthric children.
- The main stages of speech correction.
- Methods and techniques of the preparatory stage of speech correction in children diagnosed with dysarthria.
- Conclusion.
“Tell me and I will forget,
show me and I will remember
let me act on my own and I will learn.”
Confucius.
Dysarthria is an urgent, complex medical, psychological and pedagogical problem at the present stage of development of speech therapy, both for neurologists and speech therapists. Teachers of speech therapy groups are direct assistants to preschoolers in the process of joint activities with a speech therapist to eliminate severe speech disorders. Therefore, it is so important for them to know the basics of correctional pedagogy for working with children suffering from dysarthria.
Many specialists have dealt with the problem of differential diagnosis and methods of overcoming various forms of dysarthria (O.V. Pravdina, E.N. Vinarskaya, E.M. Mastyukova, L.V. Lopatina, N.V. Serebryakova, E.F. Arkhipova and others ).
E.F. Arkhipova offers five stages to eliminate erased dysarthria ( preparatory; development of new pronunciation skills;
development of communication skills; overcoming or preventing secondary disorders; preparation for school
).
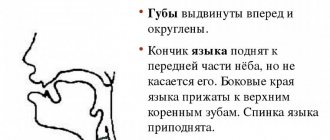
All children with dysarthria have persistent impairments in the use of their speech organs (lips, teeth, cheeks, tongue, jaws), the tongue is usually pulled back, its back is rounded and covers the entrance to the pharynx, and profuse salivation. When performing the “Spatula” exercise, children bend their lower lip with the front part of their tongue and press it down. When performing the “Reach your nose” exercise, passive movement of the anterior part of the tongue is performed with the lower lip and lower jaw. The number of impaired sounds is approximately from 8 to 10. Pronunciation defects are expressed in distorted pronunciation of sounds, especially front-lingual sounds that are difficult to articulate. Hissing sounds are articulated in the lower version, with the tongue lowered and pulled away from the lower incisors, while the tense back of the tongue helps soften them. In children with this form, soft sounds are more stable in speech than their hard pairs, a symptom of “palatalization,” that is, a “softening defect.”
The structure of dysarthric disorders includes the presence of synkinesis. The following synkinesis is most often observed in children - throwing back the head, crossing the legs, arching the body, “fanning fingers”, or bending the fingers, stretching the arms. In children, it is noted that it is impossible to simultaneously perform any movements with the hands and organs of the articulatory apparatus. Kinetic apraxia is the difficulty of smoothly transitioning from one articulatory movement to another. Kinesthetic apraxia – chaotic movements, “groping” for articulatory posture. The polymorphism of sound pronunciation disorders, the weak closure function of the cerebral cortex in children with an erased pseudobulbar form of dysarthria and the short time of correction complicate the process of formation of conditioned reflex connections in them, and as a result, control over their own speech in children of this category is practically absent. Sound production, automation and differentiation take a long time. Placed in such difficult conditions, we are forced to find the most effective ways to correct sound pronunciation in dysarthric children.
Traditionally, in domestic speech therapy, correction of sound pronunciation begins with the preparatory stage. This is the most fundamental and longest stage in children with dysarthria. “He started, he started.” It is important to note that when working with dysarthric children, this stage does not have a specific end date; it continues until articulatory patterns for all sounds are developed and the child’s ability to accurately engage certain muscles when performing a given movement is formed. Consequently, at whatever stage of sound pronunciation correction we work with dysarthric children, the preparatory stage continues. We give special preference to it, and we identify the following areas of work that can effectively and in a shorter time completely (partially) overcome violations of sound pronunciation.
We chose the words of Confucius as the epigraph to our work; they very accurately reflect the basic principle of working with children with dysarthria “... let me act on my own and I will learn.”
Directions of work of the preparatory stage in work
with dysarthric children:
1. Psychological readiness for evoking sound -
includes: the child’s interest in speech therapy classes; ability to perceive verbal step instructions.
2.Normalization of muscle tone
(training children and parents in differentiated self-massage of the face and tongue). The purpose of speech therapy self-massage is primarily to stimulate the kinesthetic sensations of the muscles involved in the work of the peripheral speech apparatus, as well as, to a certain extent, to normalize the muscle tone of these muscles.
It is important for a child to clearly imagine and reproduce articulatory movements and postures in order to consciously control their correctness, but learning such an unusual set of information is difficult for a child. He is not very interested in such information. There is visual didactic material so that each session for a child not only helps to overcome his disorder, but is also entertaining and interesting. Self-massage is carried out using various massage balls, a Su-Jok ball, which allows you to simultaneously engage fine motor skills of the hands. Exercise for self-massage of the face: “Barely, barely, barely, barely, the carousel started spinning, and then, then, then we all run, run, run...” or “We’ll draw glasses, and then stroke the cheeks.” The child accompanies simple rhyming exercises with the movements of massage balls under the control of a speech therapist, increasing or decreasing the force of stroking, pressing, tapping - this depends on the violation of muscle tone.
3.Connecting the child’s kinesthetic sensations
(when reproducing an articulation exercise, the child is guided only by his muscle sensations).
This goal is achieved using the following techniques: performing exercises without mirrors, this technique helps to emphasize the characteristics of the sounds being practiced and enhance visual feedback. The next technique is to perform articulation exercises and pronounce sounds with your eyes closed. With eyes closed while performing the exercise, the child’s attention is focused on proprioceptive sensations. You can also use the technique of touching and light pressure on parts of the face and articulatory apparatus (the “Guess” game).
4.Use of tactile-kinesthetic stimulation.
In order to stimulate kinesthesia, we use the following techniques, including finger movements on “springs”, the “Funny Springs” exercise, rubber or plastic balls with a needle surface,
clothespins
,
Su-Jok ball
, etc. When squeezing the ball or rolling it over the fingers, we activate the pronunciation of syllable rows, words with different syllabic structures, and the automation of delivered sounds.
5. Phonemic readiness to produce sound
includes: the ability to distinguish the evoked sound from those similar in sound and articulation; the ability to distinguish the evoked sound from distorted versions.
6.Work on the articulatory structure of all sounds.
When a child suffers from all groups of sounds, we “go from the child,” taking into account that the path to the correct sound is individual for each child. Therefore, you should start working on all the disturbed sounds at the same time. When performing articulation exercises and making sounds, we connect the child’s hand, it imitates the position of the articulation organs. While we are engaged in the production of one sound and consolidating it in speech, we simultaneously work on the formation of the articulatory structure of the remaining sounds. When producing several sounds at the same time, often even with the opposite pattern, it is necessary to monitor the child’s condition, dose the load, alternate with rest, so that mutual inhibition of the movements of the articulation organs does not occur. It is better to work on difficult sounds [Р], [Ш] at the same time, given that their articulatory structures are very close. If a child has interdental sigmatism, then it is better to deal with the production and automation of whistling sounds last, since they are introduced into speech longer than other sounds.
7.Connecting the hearing analyzer
. Includes the child’s ability to hear his own voice and his own pronunciation. To do this, you can use the “Mouthpiece” exercise - the child’s right hand in the shape of a “crescent” is pressed behind the right ear, slightly pointing the ear towards the mouth; the left hand in the shape of a “crescent” is located at the left side of the mouth, thus the hands form a corridor. The child performs an articulatory pattern corresponding to a given sound and pronounces it. The sound passes along the “corridor”, and the child hears his pronunciation well and can determine whether it is correct or not.
I would like to note that the described techniques make speech therapy work more interesting, varied and effective, evoke positive emotions in children and contribute to children’s greater interest in speech therapy classes.
Long-term plan for speech therapy work to correct dysarthria
Individual plan for speech therapy work
Speech therapist teacher Borodacheva I.A.
for the correction of dysarthria
I. Preparatory stage.
1. Fostering the need for correct speech.
2.Development and refinement of the child’s passive vocabulary
(what the child understands):
- carried out using plot and subject pictures, which the speech therapist names and asks the child to repeat.
3.Overcoming sensory impairments
(perception, attention, memory):
- carried out in the form of development of auditory and visual attention and perception, etc.
4. Formation of phonemic perception, differentiation of phonemes, phonemic analysis and synthesis:
- the work is similar to working on dyslalia.
5.Creating conditions on the rhythm of speech, the syllabic structure of the word:
— conditions are created in the process of exercises to develop perception and reproduce various rhythmic structures, both simple and accented.
6. Creation of conditions for the formation of general motor and articulatory skills, conditions for the formation and correction of respiratory and vocal functions:
— these conditions are created in the process of medicinal and physiotherapeutic treatment, physical therapy, massage, passive and active gymnastics.
Work on the development of the articulatory apparatus,
it is preceded by:
— carrying out differentiated massage of the facial and articulatory muscles, depending on the state of muscle tone.
The main massage techniques are stroking, pinching, kneading, and vibration. The nature of the movements will also be determined by the state of muscle tone.
— Simultaneously with the differentiated massage, work is carried out to develop facial muscles.
For this purpose, the child is taught to open and close his eyes, frown his eyebrows, nose, etc. As such tasks are completed, their differentiation and arbitrariness gradually develops.
— carrying out work to combat salivation
.
1. The child is explained the need to swallow saliva.
2. Massage the masticatory muscles, which interfere with the swallowing of saliva.
3. Inducing passive and active chewing movements, ask the child to throw his head back and an involuntary desire to swallow saliva arises; can be supported by request.
4. The child is asked to chew solid food in front of a mirror, this stimulates the movements of the chewing muscles and leads to the need to make swallowing movements, which can be reinforced with a request (i.e. from involuntary movements to voluntary ones).
5. Voluntary closing of the mouth due to passive-active movements of the lower jaws. First, passively, one hand of the speech therapist is under the child’s chin, the other is on his head, by pressing and bringing his hands together, the child’s jaws close - a “flattening” movement. Then this movement is done with the help of the child’s own hands, then actively without the help of hands, using counting and commands.
In the case of severe dysarthria, the development of speech motor skills begins with passive gymnastics, with extensive use of involuntary movements.
Work on developing lip mobility.
1. Make the child laugh (involuntary stretching of the lips).
2. Smear your lips with something sweet (“licking”
) - raising the tip of the tongue up or down).
3. Bring a long lollipop to your mouth (pull the child’s lips forward).
After these involuntary movements, they are fixed in a voluntary plan, in active gymnastics. At first, the movements will not be performed in full, not in the exact volume, then they are reinforced in special exercises for the lips (“smile”, “proboscis”, alternating them).
Work on the development of language mobility.
It begins with general movements, with a gradual transition to more subtle, differentiated movements. In case of severe dysarthria, the following exercises will be performed for articulatory gymnastics.
1. Place the tip of the tongue on the inner surface of the lower incisors.
2. Pulling the tongue forward and retracting it back.
3. Stimulation of the muscles of the root of the tongue. First, voluntarily, through reflex contractions, as a result of irritation of the root of the tongue with a spatula. Then the movements are consolidated in unconditioned reflexes, and then in voluntary “coughing” movements.
4. Performing subtle, differentiated movements of the tongue. For this purpose, movements are purposefully selected to develop the desired articulatory pattern, taking into account the normal articulation of sound and the nature of the defect. Articulatory gymnastics is best carried out in the form of games, which are selected taking into account the age of the child and the nature and degree of organic damage. Work on the formation of articulatory motor skills will be effective when it is combined with the development of general and especially manual motor skills. For this purpose, in case of severe dysarthria, a physical therapy methodologist develops the child’s supporting, grasping activities of the hands, as well as differentiated finger movements. The same work is carried out by a speech therapist during speech therapy classes, where clear finger kinesthesia is formed through special exercises and the hand is prepared for writing. You can also use various teaching aids and types of work such as squeezing and unclenching rubber bulbs, grasping small objects with your fingertips, mosaics, plasticine, drawing, tracing, shading stencils, cutting, lacing, sewing buttons, etc.
II. Stage. — Formation of primary pronunciation skills.
1. Correction of movements of the articulatory apparatus.
2. Development of articulatory praxis.
3. Development of respiratory and vocal functions.
4. Work on pronunciation (pronunciation, differentiation of sounds).
5. Work on the formation of prosodic components of speech.
6. Work on enriching the vocabulary and overcoming agramatisms.
1st 2 directions (correction of movements of the articulatory apparatus and development of articulatory praxis.).
The work begun at the 1st stage in the form of articulatory gymnastics continues, but it becomes more complicated and differentiated. If at the 1st stage the child’s basic movements are formed and consolidated, then at the 2nd stage incorrect and imprecise movements are corrected, their strength and accuracy are trained, and coordination is practiced.
In this regard, in articulatory gymnastics at the 2nd stage, differentiated movements of the articulatory organs predominate, and much attention is paid to performing a series of movements (the ability to voluntarily switch from one movement to another is assumed).
Working on breathing.
In the case of severe dysarthria, work on breathing begins with general breathing exercises. The purpose of these exercises is to increase breathing volume and normalize its rhythm. To achieve this goal, the following exercises are performed:
1. The child lies on his back, the speech therapist bends his legs at the knee joints and, with bent legs, presses on the armpits. These movements are performed in a normal respiratory rhythm and counted. This helps normalize the movements of the diaphragm.
2. The child sits, a fan of air is created in front of his nostrils. Under its influence, the depth of inspiration increases due to the inclusion of the diaphragm muscles in the work.
After active work of the diaphragm muscles, the optimal type of physiological breathing is developed. The formation of this type of breathing is carried out by imitation, in various positions, lying, sitting, standing.
The child places one hand on his diaphragm, the other on the speech therapist’s diaphragm. The speech therapist inhales and exhales, engaging the diaphragm muscles; the child, feeling the movements of his hand, tries to breathe in the same way. Then, the movements of the diaphragm, caused by imitation, are reinforced in various breathing games.
After consolidating diaphragmatic breathing, work is carried out on long, smooth exhalation through the mouth, which is carried out:
— without speech accompaniment;
— with speech accompaniment.
Work without speech support
.
It is carried out in the form of various breathing exercises using a variety of didactic aids, which allow visual control of the duration and force of exhalation through the mouth.
When performing breathing exercises, you must adhere to the following rules:
- breathing exercises should be carried out before meals, in a well-ventilated area;
- when performing breathing exercises, you should not overtire the child (the first sign of fatigue is yawning - a symptom of oxygen deficiency);
- when performing breathing exercises, it is necessary to monitor the child’s posture (straight, shoulders straightened, legs, arms calm);
- when exhaling, the child should not strain his shoulders, neck, raise his shoulders, or puff out his cheeks;
- when performing breathing exercises, the child’s attention should be drawn to the sensations of movement of the diaphragm;
— it is better to perform breathing movements smoothly, to the counting of music;
- didactic material used for breathing exercises should be light - cotton wool, thin colored paper, a balloon, etc.; it must be located at the level of the mouth.
Working with speech accompaniment.
Work is carried out while pronouncing speech material of varying complexity, with a long, smooth exhalation.
Some methodologists recommend pronunciation of vowel sounds, others - from fricative, voiceless consonants.
This work is carried out in the following exercises:
- singing vowels while exhaling - “thread”;
- pronouncing combinations of 2, 3, 4 vowels with a long, smooth exhalation (you need to make sure that there are no pauses between vowels for an additional breath);
- pronunciation of isolated fricative, voiceless consonants (when inhaling - sound);
- pronouncing fricative, voiceless consonants with a combination of vowels (sa-so-su-sy; sa-fa-ha-sha)
- pronouncing words with a smooth exhalation, at first few syllables, then many syllabics, first with emphasis on the 1st syllable, then the emphasis changes;
- constant dissemination of the phrase on a long, smooth exhalation (take a breath - then “birds” - “birds are flying” - “birds are flying in the sky” - “birds are flying in the sky to the
south”
, etc.). The number of words a child pronounces in one exhalation is determined by age:
| 5 years - | 4 – 5 words, no more |
| 6 years - | 5 – 6 words, no more |
| 7 years - | 6 – 7 words, no more |
Working on your voice.
It is carried out in parallel with work on breathing, combined with physiotherapeutic, drug treatment and differentiated massage.
In the case of severe dysarthria, the work begins with teaching the child to open and close his mouth voluntarily, since it is these movements (of the lower jaw), performed in full, that ensure normal voice formation and free vocal delivery.
To develop movements of the lower jaw, a special model is used, which is a brightly colored ball tied to a rope. The child takes the ball with his hand and at the moment of lowering his jaw, he pulls it down, then the same movement is performed with his eyes closed, in order to enhance kinesthetic sensations. Then the same movements are practiced when pronouncing vowel sounds and various sounds - imitations. After free vocal delivery is ensured and vocal constriction is relieved, voice (orthophonic) exercises are used to develop the voice. The purpose of the exercises is to develop coordination of breathing, articulatory phonation and practice the basic acoustic characteristics of the voice (strength, pitch, timbre). For example: direct counting with increasing voice or vice versa (voice strength), or ooooh
and
ooooh
, etc. (such exercises are used to develop voice pitch and modulation).
All this is practiced in special voice exercises. Voice skills are strengthened in reading fairy tales, during role-playing games, and in Russian folk tales.
Working on pronunciation.
Working on pronunciation is the main stage. Features of working with dysarthria are the following:
— Work on correcting sound pronunciation defects in dysarthria should be aimed at improving speech communication and social adaptation.
— Work on individual sounds should be carried out in a certain sequence. Start with those sounds whose articulation is most preserved. And among the defective sounds, start working with the sounds of early ontogenesis.
— When correcting sound pronunciation defects, it is necessary to take into account the influence of pathological reflexes (oral automatism).
— When correcting defects in sound pronunciation, it is also necessary to take into account the nature and distribution of spastic and poretic movements in the speech muscles.
— With severe dysarthria, at first it is not possible to achieve a clear sound, so you can move on to working on other sounds, being content with an incomplete sound frequency.
Work on pronunciation is carried out in parallel with the development of phonemic functions (phonemic perception, differentiation, phonemic analysis and synthesis). The techniques for staging, automating and differentiating sounds are the same as for correcting any sound pronunciation disorders.
Work on the prosodic side of speech.
Much attention is paid to developing the correct tempo and rhythm of speech, by learning to arbitrarily change the tempo of speech, highlight stressed syllables in the structure of a statement and correctly alternate them with unstressed syllables, and observe correct pauses.
Correction of speech tempo disorders is combined with work on the development of general movements in logarithmic classes.
The development of melodic-intonation speech is facilitated by voice exercises aimed at developing the basic tone of the statement. The tempo-rhythmic and intonation skills of speech formed in special exercises are consolidated in emotionally charged speech material (reading fairy tales, dramatizations, etc.). When selecting such material, the age of the children and the program requirements of training must be taken into account. So in preschool age it’s Barto, Marshak, etc., and in school age it’s Krylov, poems by Pushkin, Nekrasov. Older - Mayakovsky, etc.
III. Stage. – Formation of communication skills
.
1. Work continues on automation and differentiation of sounds in speech material that is more complex than at other stages.
2. Formation of pronunciation skills in various communication situations, through careful and constant expansion of the circle of communication, creating problematic situations.
3. Work continues to correct lexical and grammatical violations, and work continues with school-age children to correct reading and writing.
Features of the development of fine motor skills in children with dysarthria.
Zachupeyko Anna Valerievna
Features of the development of fine motor skills in children with dysarthria.
The concept of " fine motor skills "
means movement of hands in literal translation.
The need to develop hand motor skills in children with speech impairments , and especially those whose speech is systemically impaired, is determined by the role of fine motor skills in the formation and work of many mental processes - perception, speech, attention, and its importance in graphic and labor activities.
In the history development , the role of hands is often emphasized . It was the hands that made it possible to develop the language of communication of primitive people with the help of gestures. Research by scientists shows that hand movements arise only as a result of upbringing and training.
In addition, improving manual motor skills helps to activate various areas of the brain. In general, the level of development of motor skills is one of the important indicators of readiness for schooling. The development of fine motor skills of a person’s hand is closely related to the level of development of speech activity, therefore deficiencies in the development of this skill entail deficiencies in speech articulation, which are later reflected in the level of mastery of written speech. As is known from research in the field of speech activity in dysarthria , speech impairments are one of the important signs of this mental disorder. Consequently, motor is also the main type of abnormality in children with dysarthria .
The development of a child with dysarthria from the first days of life differs from the development of normal children . In many children with dysarthria, the development of upright posture is delayed , i.e. they begin to hold their head up, sit, stand, and walk much later. This delay in some children can be quite significant, affecting not only the entire first, but also the second year of life.
All children with dysarthria experience a decrease in interest in their surroundings, indifference, and general pathological inertia (which does not exclude loudness, anxiety, irritability, etc.)
.
They do not have a need for emotional communication with adults; as a rule, they do not have a “revitalization complex
.
normally developing child, in response to an adult’s voice or smile, throws up his arms and legs, smiles, and hums quietly, which indicates that the child has a need to communicate with an adult.
In the future, children with dysarthria have no interest in either toys hanging above the crib or toys in the hands of an adult. There is no timely transition to communication with adults based on joint actions with toys, and a new form of communication—gesture—does not arise. Children in the first year of life do not differentiate between “their own”
and
“alien”
adults, although with normal
development this occurs in them already in the first half of life.
This affects the development of the first actions with objects—grasping—and the development of perception , which is closely associated with grasping during this period. Children with dysarthria developing large and small objects differently, like objects of different shapes, as well as distinguishing the objects themselves from a number of others.
In children with dysarthria of early age, object-based activity is not formed. Some of them show no interest in objects, including toys. They do not pick up toys at all or manipulate them. Not only do they not have an orientation like “What can be done with this?”
, but also simpler orientation like
“What is this?”
.
In other cases, children of the third year of life begin to manipulate objects, sometimes reminiscent of the specific use of an object, but in reality the child, when performing these actions, does not take into account the properties and purposes of objects at all.
In addition, these manipulations are interspersed with inappropriate actions. Inappropriate actions are those actions that contradict the logic of using an object and come into conflict with the role of the object in the objective world. For example, when a child first puts a cap on the stem of a pyramid and then tries to string rings; knocks the doll on the table; trying to fit a large car into a small garage, etc. Such actions add nothing to knowledge.
The presence of inappropriate actions is a characteristic feature of a child with dysarthria .
The actions of children with dysarthria with objects represent manipulations that are similar to those of younger, normally developing children , but are interspersed with inappropriate actions that are not typical for normal children .
At the same time, the development trends of a child with dysarthria are the same as those of a normally developing child . Much in the development of a child—a lag in mastering objective actions, lag and systemic deviations in the development of speech and cognitive processes—is largely of a secondary nature. With proper organization of the life of a child with dysarthria , requiring the earliest possible inclusion of special education, many developmental can be corrected and even prevented.
Development in preschool age is, as is known, a continuation of the development that we observe at an early age. Despite the fact that at 3 years a certain leap occurs, further development is based on the level that was achieved before. At the same time, this age has its own characteristics , its own tasks, many of which arise for the first time.
In early preschool age, children mainly master specific manipulations, which should form the basis for the formation of visual-motor coordination and the identification of properties and relationships of objects. However, the process of mastering specific manipulations without special training is slow, since children do not develop a genuine interest in the objective world around them. interest in objects , in particular toys, turns out to be short-lived, as they are stimulated only by their appearance. Along with nonspecific manipulations, children of the fourth year of life exhibit a large number of inappropriate actions with objects. Their number sharply decreases only in the sixth year, giving way to specific manipulations leading to familiarization with the properties and relationships of objects.
It should also be noted that younger preschoolers with speech disorders have underdevelopment of the motor sphere and, above all, fine motor skills . Children's movements are poorly coordinated, imprecise, many of them do not hold objects well, and often operate with one hand. Some children are not capable of quickly changing motor settings . Some preschool children with dysarthria have a lack of muscle strength, rhythm of voluntary movements, and tempo. A violation of verbal regulation of actions is also detected, which manifests itself in difficulties when performing tasks following verbal instructions.
For children with dysarthria, preschool age is the beginning of the development of perceptual action. Based on the child’s awakened interest in objects and toys, an acquaintance with their properties and relationships arises. The fifth year of life becomes a turning point in the development of perception of a child with dysarthria .
However, the problems that were observed in the development of fine motor skills as the sensory basis of perceptual action continue to occur in a preschooler with dysarthria , but due to the complication of activity they become even more profound. At this age, disturbances in manual motor skills no longer appear at the level of individual actions, but at the level of complex sets of movements, as well as at the level of visual-motor coordination of movements, which means that fine differentiated movements of the hands and fingers are especially difficult in children with dysarthria They have difficulty learning to lace up their shoes, tie shoelaces, and fasten buttons; they often do not measure their efforts when handling objects: they either drop them, or squeeze them too hard, or pull them.
Fine motor skills disorders manifest themselves in productive activities: manual labor and visual arts. Often, a child with dysarthria actively turns the sheet of paper when drawing or coloring. This means that the child replaces the ability to change the direction of a line with fine finger movements by turning the sheet, depriving himself of finger and hand training. It is also quite common in practice to encounter such a feature of the visual and graphic activity of a preschooler with dysarthria , when he draws objects that are too small, which, as a rule, indicates a rigid fixation of the brush when drawing. When modeling, a child often cannot control the force of pressure, his movements are chaotic, imprecise, and there is no voluntary control of movements. During work, the child has difficulty performing subtle and precise actions, coordination of movements, and hand strength is either insufficient or poorly controlled. A serious drawback that causes many problems in the development of fine motor skills in children is the lack of self-control over actions, disturbances in the tempo of actions (hasty or slowness)
etc.
as indicators of pathological disorders in the development of fine motor skills in dysarthria .
Stiff hand movements
If a six-month-old child still holds one or both hands clenched into a fist, this is a warning signal for parents and teachers. Sometimes the hands are squeezed so tightly that an adult can hardly insert a rattle into the child’s palm.
Between the 6th and 12th month, the baby should begin to play with his fingers in such a way that each finger actively moves. Children with developmental have difficulty moving individual fingers.
The baby reaches for the object, but he has difficulty grasping and holding it. It is often difficult for an older child to grasp something in his hands, for example, a talking doll, a squeaking rubber toy, etc.
Unilateral fine motor
To recognize disorders at an early stage, great attention must be paid to unilateral weakness or immobility of the hands and fingers. If an older child, in the process of demonstrating tendencies towards right- or left-handedness, prefers one hand, there is no pathology in this. But if a child, when working with objects, never resorts to the help of his second hand, this is a serious suspicion of a unilateral functional disorder.
Cramps and trembling
Sharp and repeated muscle contractions in the child’s hand will be noticeable. Similar convulsive movements can also occur in the area of the forearms, shoulders, and the back of the head (convulsive jerking of the head)
or faces
(facial convulsions)
.
Convulsive twitching of the whole body is sometimes mistaken for shuddering from fear, but their causes may be a violation of the central nervous system.
Sometimes you can observe not impetuous, but slow and pulling movements of the fingers and hands. They, just like convulsions, do not obey the will. In this case, the fingers sometimes perform twisting, worm-like movements. Similar slow and tense movements can be observed in the facial muscles.
described above appear more often in older children . These also include trembling in the hands and fingers during passive and active movements. As a consequence of this, there is uncertainty when grasping objects. A small child who begins to draw cannot make even strokes.
Smaller or larger tremors may also appear in the muscles of the head and body .
When the tongue moves, children with dysarthria often experience accompanying movements of the fingers of the right hand (
especially the thumb) (syncinesia)
.
The development of fine motor skills is of great importance for the development of speech , so normal finger and hand movements are extremely important for children with speech disorders .
fine motor skills deficiencies occurs through children performing a large number of exercises aimed at developing dexterity , accuracy, simultaneity (synchrony)
finger movements.
So, in general terms, the patterns of mental development coincide for normative children and children with deviations . However, there is something specific in the development of children with speech disorders. The development of a child with dysarthria from the first days of life differs from the development of normal children . The actions of children with dysarthria with objects represent manipulations that are similar to those of younger, normally developing children , but are interspersed with inappropriate actions that are not typical for normal children .
Children's movements are poorly coordinated, imprecise, many of them do not hold objects well, and often operate with one hand. Some children are not capable of quickly changing motor settings . Some preschool children with dysarthria have a lack of muscle strength, rhythm of voluntary movements, and tempo. A violation of verbal regulation of actions is also detected, which manifests itself in difficulties when performing tasks following verbal instructions. Later, disturbances in manual motor skills no longer appear at the level of individual actions, but at the level of complex sets of movements, as well as at the level of visual-motor coordination of movements.
Let's consider the features of fine motor skills in its most common form - erased dysarthria .
According to research by L.V. Lopatina, preschoolers with an erased form of dysarthria have impairments in manual motor skills , manifested mainly in impaired accuracy, speed and coordination of movements. causes significant difficulties in children . In most cases, it turns out to be difficult or impossible to quickly and smoothly reproduce the proposed movements. In this case, additional movements, perseverations, rearrangements, and impaired optical-spatial coordination are noted. Switching movements is often carried out in conjunction, according to verbal instructions and with pronouncing their sequence. The most impaired is the ability to simultaneously perform movements, which indicates a certain dysfunction of the premotor systems , which primarily provide the kinetic organization of movements
Thus, it was found that the majority of children with an erased form of dysarthria had mild (erased)
neurological symptoms, which were revealed upon careful examination and indicated organic damage to the central nervous system.
Children with erased dysarthria are motorically awkward , the range of active movements is limited, and the muscles quickly tire under functional loads. They stand unsteadily on one leg, cannot jump on one leg, or walk along a “bridge”
etc. They imitate movements poorly: how a soldier walks, how a bird flies, how bread is cut, etc.
Motor incompetence is especially noticeable in physical education and music classes, where children lag behind in the tempo, rhythm of movements, as well as in switchability movements.
Children with erased dysarthria late and have difficulty mastering self-care skills: they cannot button a button, a scarf, etc. d. During drawing classes, they do not hold a pencil well, their hands are tense. Many people don't like to draw. Motor clumsiness of the hands is especially noticeable during applique classes and with plasticine. In works on appliqué, difficulties in the spatial arrangement of elements can also be traced. Violation of fine differentiated movements of the hands is manifested when performing sample tests of finger gymnastics. Children find it difficult or simply cannot perform an imitation movement without assistance, for example, a “lock”
- put your hands together, intertwining your fingers;
“rings”
- alternately connect the index, middle, ring and little fingers with the thumb and other finger gymnastics exercises.
During origami classes they experience enormous difficulties and cannot perform the simplest movements, since both spatial orientation and subtle differentiated hand movements are required. According to mothers, many children under 5-6 years old are not interested in playing with construction sets, do not know how to play with small toys , and do not assemble puzzles.
The general motor sphere of children with an erased form of dysarthria is characterized by awkward, constrained, undifferentiated movements. There may be a slight restriction in the range of movements of the upper and lower extremities; with functional load, concomitant movements are possible (syncenesis, disturbances in muscle tone. Often, with pronounced general mobility, the movements of a child with an erased form of dysarthria remain awkward and unproductive.
Insufficiency of general motor skills manifested in preschoolers with this disorder when performing complex movements that require precise control of movements, precise work of various muscle groups, and correct spatial organization of movements. For example, a child with an erased form of dysarthria , somewhat later than his peers, begins to grasp and hold objects, sit, walk, jump on one or two legs, runs awkwardly, and climbs on a wall bars. In middle and senior preschool age, it takes a long time for a child to learn to ride a bicycle, ski and skate.
In children with an erased form of dysarthria disturbances in fine motor skills of the fingers , which are manifested in impaired accuracy of movements, a decrease in the speed of execution and switching from one pose to another, slow initiation of movement, and insufficient coordination. Finger tests are performed imperfectly, and significant difficulties are observed. These features are manifested in the child’s play and learning activities. A preschooler with mild manifestations of dysarthria is reluctant to draw , sculpt, or play ineptly with mosaics.
Features of the state of general and fine motor skills are also manifested in articulation, since there is a direct relationship between the level of development of fine and articulatory motor skills .
age children in the first grade experience difficulties in mastering graphic skills (some experience “mirror writing”
;
replacing the letters “d”
-
“b”
; vowels, word endings; bad handwriting; slow pace of writing, etc.).
With pseudobulbar palsy, different muscles are not affected to the same extent: some more, others less.
Clinically, paralytic, spastic, hyperkinetic, mixed and erased forms of the disease are distinguished. Most often, mixed forms occur, when the child has all the phenomena of motor impairment - paresis , spasticity and hyperkinesis.
Paresis manifests itself in the form of lethargy, decreased strength of movement, its slowness and exhaustion, any movement is made slowly, often not completed, repeated movement is made with even greater difficulty, and sometimes cannot be repeated at all.
Specific development of fine motor skills is also observed in cerebellar dysarthria . Considering cerebellar dysarthria , it can be noted that the function of the cerebellum is known to be:
1) has a significant impact on muscle activity, regulating the correctness and coordination of movements;
2) affects the coordination of movements of the muscles of the vocal apparatus.
The cerebellum controls and regulates muscle tone, and when it is damaged, dissemetry occurs, expressed in improper muscle contraction. In general, there is a lack of coordination of movements. The gait becomes unsteady, and the patient has difficulty maintaining balance. There are a number of neurological tests to identify dysfunctions of the cerebellum.
The next form of dysarthria , in which specific disorders of fine motor skills are observed, is bulbar dysarthria . Bulbar dysarthria is a symptom complex of speech motor function disorders that occurs in various diseases of the medulla oblongata in which damage occurs (both unilateral and bilateral)
the motor nuclei of the cranial nerves located in it
(VII, IX, X, XII pairs)
or their roots and peripheral parts.
With bulbar dysarthria, peripheral paresis is observed, sometimes to the extent of paralysis.
The development of pseudobulbar dysarthria occurs with bilateral damage to the motor corticonuclear pathways running from the cerebral cortex to the nuclei of the cranial nerves of the brain stem. With pseudobulbar dysarthria , voluntary movements are most affected.
Pseudobulbar dysarthria is characterized by the development of increased muscle tone in the muscles, similar to spasticity. dysarthria occurs . Much less often, when there is a limitation on the volume of possible voluntary movements, an unexpressed increase in muscle tone in certain muscle groups is observed or, on the contrary, a decrease in muscle tone - in this case they speak of a paretic form of pseudobulbar dysarthria . It should be noted that in both forms there is a significant restriction of voluntary, active movements of the articulatory muscles, and in severe cases, an almost complete absence of such movements. Dysarthric children are unable to care for themselves. Such a child cannot put on clothes and shoes on his own. He runs and jumps poorly. motor skills and fine coordination of movements are primarily affected here.
Signs of pseudobulbar syndrome can be detected already in a newborn. Such first manifestations of pseudobulbar syndrome are weakness or absence of cry (aphonia, disturbances in the acts of sucking, swallowing, absence or pronounced weakness of a number of innate unconditioned reflexes, which include sucking, searching, proboscis and palmar-orocephalic reflexes.
Let's consider the specifics of the development of fine motor skills in the extrapyramidal form of dysarthria . Subcortical, or extrapyramidal, dysarthria develops as a result of various lesions of the subcortical nuclei of the brain, as well as nerve fibers that connect the subcortical nuclei with other structures of the brain, which include the cerebral cortex. The extrapyramidal system provides the existence of a background for the implementation of precise, fast, differentiated and coordinated movements. The extrapyramidal system, through communication with other parts of the nervous system, plays a significant role in maintaining and regulating muscle tone, the strength of muscle contractions, maintaining the sequence of muscle contractions and movements, and ensures the automated execution of complex movements.
The main manifestations are extrapyramidal disorders of muscle tone such as hypertension, hypotension or dystonia.
With extrapyramidal, or subcortical, dysarthria , violent movements are observed (hyperkinesis, various disorders of the formation and conduction of proprioceptive nerve impulses from the muscles of the speech apparatus to the structures of the central nervous system, emotional-motor innervation also suffers. Extrapyramidal disorders manifest themselves mainly as pathogenetically interrelated disorders of the muscle tone (rigidity or hypotonia)
and movement disorders
(hyperkinesis or hypokinesis)
. In the striatal system there is a somatotopic distribution: the head is represented in the oral sections, the arm in the middle, and the torso and leg in the caudal sections. Therefore, when one or another part of the striatum is damaged, violent movements occur in the corresponding muscle groups.
The clinic distinguishes between diseases caused by damage to the predominantly phylogenetically old or new part of the extrapyramidal system. New part of the extrapyramidal system (neostriatum)
has a mainly inhibitory effect on the old (pallidonigral, therefore, when the function of the neostriatum falls out or decreases, the old part of the extrapyramidal system seems to be disinhibited and the patient begins to have violent movements; with a simultaneous decrease in muscle tone,
a hyperkinetic-hypotonic syndrome develops (with choreic hyperkinesis)
.
When the old part of the extrapyramidal system is damaged, the opposite picture occurs. Patients experience slowness and poverty of movements with a simultaneous increase in muscle tone - hypokinetic-hypertensive (akinetic-rigid) develops
syndrome or parkinsonism syndrome, an important link in the pathogenesis of which is considered to be insufficiency of the dopaminergic systems of the brain, primarily dopamine and increased activity of its biochemical antagonist - acetylcholine, which
promotes the release of histamine and inhibition of cholinesterase.
Stiffness, increased tone of all muscles, bradykinesia, bradyllalia, facial and gestural poverty, and lack of accompanying movements are noted. Against the background of general stiffness and stiffness of the muscles, tremor of the fingers is observed, often affecting the lower jaw and tongue. The following types of hyperkinesis are distinguished.
Chorea is characterized by polymorphic rapid violent movements involving the muscles of the limbs, trunk, neck and face. In this case, hyperkinesis is irregular and inconsistent, with a rapid change in the localization of convulsive twitches, intensifies with excitement and disappears in sleep. Reflexes are not changed.
Characteristic of choreic hyperkinesis is the occurrence of rapid involuntary movements against the background of muscle hypotension (hyperkinetic-hypotonic syndrome)
.
Choreic hyperkinesis is observed during low (night)
chorea, Huntington's disease.
Athetosis, or mobile spasm, is hyperkinesis, which is manifested by violent slow worm-like movements with alternating hyperextension and flexor movements mainly in the distal limbs. With this hyperkinesis, the phase of muscle hypotonia is replaced by a phase of a sharp increase in tone. From time to time, a general tonic spasm of all muscles of the limbs may occur.
A tic is a stereotypically repetitive clonic spasm of a single muscle or group of muscles, usually the muscles of the neck and face. In contrast to neurotic reversible tics, extrapyramidal tics are characterized by consistency and stereotyping.
Myoclonus is a short, lightning-fast clonic twitching of individual muscles or muscle groups so fast that there is no movement of the limbs in space. Myoclonus is most often observed in the muscles of the trunk and less often in the limbs, intensifying with excitement and physical stress.
Hemiballismus - as a rule, unilateral rough, tossing, sweeping movements of the limbs, often the hands, are observed, usually carried out by proximal muscle groups. Hemiballismus occurs when the subthalamic nucleus (corpus Luis)
as a result of tuberculoma, syphilitic gumma, metastatic abscess, encephalitis, most often as a result of vascular disorders
(thrombosis, hemorrhage, embolism)
.
The listed types of hyperkinesis are often combined, for example, choreic movements and torsion spasm or athetosis (choreo-athetosis)
.
Trembling (tremor)
- very fast rhythmic
(4-6 oscillations per 1 s)
, low-amplitude violent movements, characterized by alternating flexion and extension in various joints.
In contrast to intention tremor, when the cerebellum is damaged, extrapyramidal tremor is more pronounced at rest and decreases or even disappears with active movements (static tremor)
.
A characteristic feature of hyperkinesis caused by damage to the estrapyramidal system is that they disappear during sleep, and intensify with excitement and voluntary movements.
Let's consider violations of fine motor skills in the cortical form of dysarthria . Depending on the location of the lesion in the cerebral cortex, two types of cortical dysarthria . The first type is cortical kinesthetic postcentral dysarthria (some authors call this type afferent cortical dysarthria ). It occurs due to damage to the postcentral gyrus of the cerebral cortex. As a rule, brain damage is unilateral, and the dominant, most often the left, hemisphere of the brain is affected.
The basis of cortical kinesthetic dysarthria is apraxia of the kinesthetic type. In addition to kinesthetic dyspraxia of the articulatory apparatus, dyspraxia of the kinesthetic type is noted in both the speech muscles and the muscles of the fingers.
Fine motor skills disorders pronounced in productive activities: manual labor and visual arts.
So, intensive physiological development of the hand as an organ occurs during the first three years of a child’s life, and this development must necessarily be accompanied by a special pedagogical organization; It has been established that the effectiveness of his further education largely depends of development
Dysarthria is a Latin term that means a disorder of articulate speech and pronunciation. In practice, a slightly different understanding of this term has developed - as a disorder of the motor motor side of oral speech .
With dysarthria at different levels, the transmission of impulses from the cerebral cortex to the nuclei of the cranial nerves is disrupted. In this regard, to the muscles (respiratory, vocal, articulatory, as well as muscles of the limbs)
nerve impulses do not arrive, the function of the main cranial nerves directly related to speech is disrupted.
As is known from research in the field of speech activity in dysarthria , speech impairments are one of the important signs of this mental disorder. Consequently, motor is also the main type of abnormality in children with dysarthria .
At the same time, lesions of different areas and zones of the brain lead to a significant variety of fine motor skills disorders in children with dysarthria of various forms - from coordination disorders to paralysis and paresis of the limbs.
Bibliography
1 Aksenova M. Development of fine movements of the fingers in children with speech disorders . / Preschool education. 1990. No. 8 - P. 62 –65.
2 Current problems in diagnosing mental retardation / Ed . Lebedinskaya K.S. - M.: Education, 1982.
3 Bogateeva Z. A. Preparing a child’s hand for writing in drawing classes. / Preschool education. 1987. No. 8. – P. 32 – 43
4 Boryakova N. Yu. Early diagnosis and correction of mental retardation . – M.: “Gnome-Press”
, 2000.
5 Vinarskaya E. N. Early speech development of a child and problems of defectology. - M.: Publishing House "Sfera"
, 1997.
6 Gavrilushkina O. On the organization of education of children with mental retardation // Preschool education. - 1998 - No. 2 - p. 67-71
7 Gastev A.K. How to work. Practical introduction to the science of labor organization. - M.: Economics, 1972. - 478 p.
8 Gorshkova E. V. Development of the motor sphere and the manifestation of emotional states in it. /Teacher's Diary: Development of Preschool Children . / Ed. O. M. Dyachenko, T. V. Lavrentieva. Ed. 2nd. – M.: Academy, 1999. – P. 45-55
9 Zhurba L. T. Mastyukova E. M. Impaired psychomotor development of children in the first year of life . - M.: Medicine, 1981. - 272 p.
10 Zaporozhets A.V. Development of voluntary movements. - M.: APN RSFSR, 1960. - 430 p.
11 Ivanichev G. A. Clinical lectures on the neurophysiology of acupuncture. - Kazan, 1994. - 48 p.
12 Kistyakovskaya M. Yu. Development of movements in children of the first year of life . - M.: Pedagogy, 1970. - 222 p.
13 Koltsova M. M. A child learns to speak. — M.: “Soviet Russia”
, 1973. – 112 p.
14 Koltsova M. M. Movement and development of motor speech . - M.: Education, 1973. - 96 p.
15 Koltsova M. M., Ruzina M. S. A child learns to speak: Finger play training. - St. Petersburg: Rech, 1998. – 245 p.
16 Korvat A.I. Psychophysiological mechanisms of movement of fingers and hands when constructing written characters. - M., 1971. — 17 s.
17 Correctional education as the basis for the personal development of abnormal preschoolers. /Edited by Noskova L.P. - M.: Education, 1989.
What to do if a child is diagnosed with dysarthria: advice from a speech therapist
Some parents are faced with the fact that their child - natural or adopted - has speech problems and, hearing the word “dysarthria”, feel confused. What is dysarthria, why does it occur and how to correct it, says Resource specialist, speech therapist of the highest category, member of the Russian Dyslexia Association Galina Orlova.
− Dysarthria is a disorder of the pronunciation side of speech, which is associated with damage to the central part of the speech motor analyzer and a violation of the innervation of the muscles of the articulatory apparatus. Simply put, the child cannot fully perform the movements necessary for speech. Sound pronunciation suffers from this, explains Galina. - In milder cases, this is a distortion of certain sounds. In severe cases of the diagnosis, omissions and replacement of sounds may be noticed. The pace and expressiveness of speech are impaired.
Dysarthria can also be characterized by the presence of paralysis and paresis of the organs of articulation. In this case, incomprehensible speech is a consequence of the diagnosis, up to the absence of speech due to complete paralysis of the speech motor muscles - anarthria.
The causes of dysarthria can be different - deviations from the norm during intrauterine development due to toxicosis, hypertension, nephropathy in the mother, infectious diseases suffered by a woman during pregnancy, as well as asphyxia of newborns, rapid or prolonged labor, mechanical obstetrics, a long anhydrous period in childbirth
From the very first days of life, such children are observed by a neurologist. They are often prescribed medication, massage and other rehabilitation procedures.
− How to recognize dysarthria?
− An attentive parent may suspect it by the child’s unusual facial expressions, profuse salivation, the shape and position of the tongue, the ability to fix an articulatory position, and sound pronunciation.
− When should you start working with dysarthrics?
− It is advisable to begin speech therapy work with any speech disorder in early preschool age. The earlier the disease is diagnosed, treatment and corrective classes are started, the greater the chances of success.
− What should parents do if their child is diagnosed with dysarthria?
— The first step, of course, is an examination by a neurologist. There are no special medications to combat dysarthria. The doctor only corrects some neurological symptoms with the help of medications. It is also important to consult a speech therapist who knows the technique of speech therapy massage, who, after a full examination, will give a conclusion and recommendations.
In addition, experts advise developing fine motor skills. You can assemble puzzles and Lego sets, sculpt from plasticine - there are many games that develop little fingers. You can use non-traditional methods of influence, such as su-jok therapy. The simplest method of su-jok therapy is training with special massage balls.
Logorhythmics classes are recommended for children two to three years old, for example, according to Zheleznova’s method. To correct dysarthria in children five years old, a speech pathologist is involved in the classes.
− What is the focus of the speech therapist’s work in the classroom?
— The specialist is engaged in the development of the prosodic side of speech - rhythm, strength, timbre, melody, tempo, logical stress, diction, as well as articulation and sound pronunciation, auditory attention, phonemic hearing, correction of speech breathing. The speech therapist will also pay attention to the normalization of muscle tone in the articulatory muscles and the development of voluntary facial movements.
If you do not have the opportunity to visit a speech therapist, then you can work with your child at home on your own, having previously completed a course with a specialist.
I will give examples of some elements of speech therapy massage and self-massage: take turns puffing out our cheeks, retracting our cheeks; close and open your mouth, click your teeth; suck on a small piece of sugar or candy; imitate the resorption of a lollipop; lick your lips; We hold a piece of bandage or gauze with our teeth for a long time; the adult’s task is to try to carefully remove the fabric.
It is also important to perform a complex of articulatory gymnastics - these are the “Proboscis” exercises (pull your lips forward, teeth and lips are closed, hold for five seconds), “Fence” (lips in a smile are tense with the mouth slightly open, teeth are clenched, the lower jaw is in a calm state, hold for five seconds) and their alternation, “Window” (with each count we open and close our mouth), “Spatula” (when smiling with an open mouth on a relaxed lower lip, place the tongue flat, hold for five seconds), “Needle” (smile with an open with our mouth, we put our tongue forward, trying not to bend it upward), “Needle shovel” (alternating exercises), “Clock” (we smile with our mouth open, stick out our tongue and make movements to the right and left, while touching the corners of our mouth with our tongue), “ “Swing” (smile with an open mouth, the tip of the tongue resting either on the upper or lower teeth), “Horse” (we click the tip of the tongue, imitating the clatter of hooves).
Over the years of work, I have often met children diagnosed with dysarthria of varying severity. This type of speech disorder has become a global problem in recent years, so it is extremely important to identify disorders in time and consult a specialist. But parents should know that correctional work with dysarthric children should not be limited to classes with a speech therapist. For the best results, this work should be continued at home, on a walk and in any joint activities.
Press service of the Department of Labor and Social Protection of the Population of Moscow
Corrective work for erased dysarthria
Erased form of dysarthria
– one of the most common and difficult to correct disorders of pronunciation of speech in children of preschool and primary school age. The number of children with an erased form of dysarthria has especially increased in recent years, which was noted during my work in the Zaslavsky school and Minsk.
With minimal dysarthric disorders, there is insufficient mobility of individual muscle groups of the speech apparatus (lips, soft palate, tongue), general weakness of the entire peripheral speech apparatus due to damage to certain parts of the nervous system. Today it can be considered proven that in addition to specific disorders of oral speech, there are deviations in the development of a number of higher mental functions and processes responsible for the development of written speech, as well as a weakening of general and fine motor skills.
Children with erased dysarthria have some characteristic features. In early childhood, they speak unclearly and eat poorly. They usually do not like meat, carrots, or hard apples as they find it difficult to chew. After chewing a little, the child can hold the food in his cheek until adults reprimand him. It is more difficult for such children to develop cultural and hygienic skills, which require precise movements of various muscle groups. The child cannot rinse his mouth on his own, because... his tongue and cheek muscles are poorly developed. Children with dysarthria do not like and do not want to fasten their own buttons, lace up their shoes, or roll up their sleeves. They also experience difficulties in visual arts: they cannot hold a pencil correctly, use scissors, or regulate the pressure on the pencil and brush. Such children also have difficulty performing physical exercises and dancing. It is not easy for them to learn to correlate their movements with the beginning and end of a musical phrase, and to change the nature of movements according to the beat. They say about such children that they are clumsy because they cannot clearly and accurately perform various motor exercises. It is difficult for them to maintain balance while standing on one leg, and they often do not know how to jump on their left or right leg.
With erased dysarthria, sound pronunciation disorders are caused by violations of phonetic operations, therefore the development of articulatory motor skills becomes the most important area of correctional speech therapy work. In my work, I carry out a differentiated approach to each child, and also adhere to two directions of correctional work: 1. formation of the kinesthetic basis of movement:
feeling the position of the organs of articulation;
2. formation of the kinetic basis of movement:
the movements of the tongue and articulatory organs themselves.
The defining moment in sound production is the formation of static-dynamic sensations, clear articulatory kinesthesia and a kinesthetic image of the movements of articulatory muscles. The work must be carried out with maximum connection of all analyzers. Shakhovskaya S.N. recommended using all analyzers in speech therapy classes. The same thing should be said, depicted, looked at, i.e. pass through the “gate” of all senses. The success of working on sound is determined by the ability to form conscious kinesthetic supports in children. It is important that the child can feel the position and movements of the articulatory organs at the moment of articulation (for example, the rise of the back of the tongue when pronouncing [k], [g]). It is necessary to take into account various tactile sensations (primarily tactile vibration and temperature), for example, the feeling of vibration in the hand in the area of the larynx or crown when pronouncing voiced consonants, the duration and smoothness of the exhaled stream when pronouncing fricative sounds [F], [V], [X], brevity of articulation, sensation of a push of air when pronouncing stop consonants [P], [B], [T], [D], [G], [K], sensation of a narrow stream of air [S], [Z], [F], wide [T], [K], temperature [C] – cold jet, [W] – warm.
When producing sounds, it is important that children know the articulatory structure of sound, be able to tell and show in what position the lips, teeth, tongue are, whether the vocal folds vibrate or not, what is the strength and direction of the exhaled air, the nature of the exhaled stream. It is useful to compare speech sounds with non-speech sounds. Such conscious mastery of correct articulation is of great importance for the formation of the correct articulatory image of the sound of its pronunciation and, most importantly, its differentiation from other sounds.
When forming the kinetic basis of articulatory movements, the main attention should be paid to exercises aimed at developing the necessary quality of movements: volume, mobility of the organs of the articulatory apparatus, strength, accuracy of movements, and developing the ability to hold the articulatory organs in a given position. Traditional articulation exercises are widely used to develop dynamic coordination of movements, but special sets of exercises that take into account the specifics of the disorder also give good positive results.
For children with mild dysarthria and increased muscle tone in the articulatory muscles, exercises are offered to relax tense muscles of the tongue and lips.
To relax the tongue
:
- stick out the tip of your tongue. Mash it with your lips, pronouncing the syllables pa-pa-pa-pa - then leave your mouth slightly open, fixing your wide tongue and holding it in this position, counting from 1 to 5-7;
- stick the tip of your tongue out between your teeth, bite it with your teeth, pronouncing the syllables ta-ta-ta-ta, leaving your mouth slightly open on the last syllable, fixing the wide tongue and holding it in this position, counting from 1 to 5-7 and return to its original position;
- open your mouth, place the tip of your tongue on your lower lip, fix this position, holding it while counting from 1 to 5–7, return to its original state;
- silently pronounce the sound I, while simultaneously pressing the lateral edges of the tongue with your lateral teeth (this exercise is also a kind of massage technique for paretic condition of the muscles of the lateral edges of the tongue)
To lower a tense tongue root
Exercises involving tongue protrusion are suggested.
Relaxing tense lips
achieved by lightly patting the upper lip on the lower lip.
In case of decreased muscle tone
preschoolers with mild dysarthria are offered tasks to activate and strengthen paretic muscles:
– scratching with the tip of the tongue on the upper incisors;
– counting the teeth, resting the tip on each one;
– stroking the cheek with the tip of the tongue, pressing forcefully on its inner side;
– holding a round piece of candy at the alveoli with the tongue.
Lips that do not close tightly, flaccidly are trained using the following tasks:
– stretch your lips into a smile, exposing the upper and lower incisors, holding the count from 1 to 5–7, return to their original position;
– stretch only the right and left corners of the lip in a smile, exposing the upper and lower incisors, hold the count from 1 to 5–7, return to the original position;
– hold pieces of crackers, tubes of different diameters, strips of paper with your lips;
- tightly closed lips.
And for the little ones (from three years old)
You can use the following types of exercises, which can be done in a playful way.
Exercises will help develop the mobility of articulatory muscles and promote the development of clear diction. You can start practicing with these articulation exercises if you have erased dysarthria. To make it interesting for children to do the exercises, their names are presented in a playful way.
"Fence"
- Teeth closed, smile broadly and show upper and lower teeth. Maintain the position for 10 seconds, repeat 3-4 times.
"Tube"
- teeth are closed, lips are pulled forward so that they resemble an “elephant’s trunk”, while the lower jaw remains motionless. Hold the position for 10 seconds, repeat 3-4 times.
"Pancake"
- open your mouth, place your wide and spread tongue on your lower lip. Maintain the position for 10 seconds, repeat 3-4 times.
"Needle"
- open your mouth and stick your sharp tongue out of your mouth as far as possible. Hold the position for 5 seconds, repeat 3-4 times.
"Pancake - a needle"
- alternate the 2 previous exercises, while ensuring that the lower jaw remains motionless. Perform the exercise at a slow pace, repeat each movement 4 times.
"Pendulum"
- open your mouth, alternately touch your sharp tongue to the right and then to the left corner of your mouth. Make sure that the lower jaw remains motionless. Perform the exercise at a slow pace, repeat each movement 4 times.
"Swing"
- open your mouth, alternately touch your sharp tongue to the upper lip, then to the lower. Make sure that the lower jaw remains motionless. Perform the exercise at a slow pace, repeat each movement 4 times.
"Let's lick our lips"
- open your mouth, lick in a circle first the upper, then the lower lip. Make sure that the lower jaw remains motionless. Repeat the exercises in a circle 4-5 times.
"Vanka-Vstanka"
- open your mouth, bend the tip of your tongue as far as possible to the base of the upper incisors, then bend the tongue to the base of the lower incisors. Perform the exercises at a slow pace, repeat the movements in each direction 4 times.
Thus, in order to carry out successful correctional work with children with an erased degree of dysarthria, it is necessary to highlight the main aspects: To identify an accurate speech therapy conclusion, a thorough psychological, medical and pedagogical examination is necessary with the study of the child’s medical record, familiarization with anamnestic data, and a doctor’s conclusion. It is necessary to maintain a close relationship with parents, not only in order to obtain information about the early development of the child, but in order to explain the characteristics of this disorder.
Implementation of a differentiated approach to overcoming dysarthria, with increased or decreased muscle tone.
An important factor in working with children with an erased degree of dysarthria is the formation of clear static-dynamic sensations of articulatory muscles. Systematicity in the work on the formation of phonemic operations, the development of the melodic-intonation side of speech, breathing processes, voice formation, articulation. The communicative focus of training is the use of story-based, didactic games, and project activities in the process of automating sound pronunciation.
Literature:
1. Arkhipova E.F. Correctional and speech therapy work to overcome erased dysarthria. – M., 2008.
2. Kiseleva V.A. Diagnosis and correction of the erased form of dysarthria. – M., 2007.
3. Lopatina L.V., Serebryakova N.V. Overcoming speech disorders in preschool children. – St. Petersburg, 2001.
4. Fedosova O.Yu. Conditions for creating a strong sound pronunciation skill in children with mild dysarthria. – Speech therapist in kindergarten No. 2, 2005.
5. www.logoped-therapy.com (Rusina Yu.V. Articulation gymnastics for clear pronunciation)
6. www.festival.1september.ru (Komarova A.A. Erased form of dysarthria in preschool children)