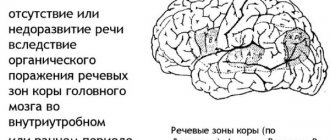
Dysarthria is a speech disorder. It occurs due to damage to the parts of the brain that are responsible for connections with the articulatory apparatus. One of the most common and simplest forms is erased dysarthria. It is diagnosed when the child reaches 5 years of age. The baby's speech is slurred, he distorts or replaces sounds, he has poor diction - these are the signs of this disease.
In the article we will talk about correctional work for dysarthria, features of sound production, complex treatment and prevention of the disease.
Principles of speech correction for dysarthria
Speech therapists use several principles when working with children. Here they are:
- Individual approach. The specialist evaluates the compensatory capabilities of the little patient - what articulatory movements have been preserved, what sounds and syllables the baby pronounces correctly;
- From simple to complex. Correction always begins with those sounds that the child pronounces best. This sequence of sound production for dysarthria allows you to achieve better results.
- Long practice of each sound. Speech correction in children with dysarthria requires much more time than other speech therapy problems.
Corrective work includes the following stages: production, automation and differentiation of sounds. But the very first task of a speech therapist is to teach the child to distinguish them by ear.
Speech therapy massage according to Prikhodko
Speech therapy massage is an active method of mechanical influence for dysarthria. It is used in cases where there is a violation of the tone of the articulatory muscles, changing the condition of the muscles of the peripheral speech apparatus. It indirectly helps improve the pronunciation side of speech.
Speech therapy massage according to Prikhodko is carried out at all stages of corrective action. It is used in the initial stages of rehabilitation, when the patient still does not have the fundamental ability to perform certain articulatory movements. Differentiated speech therapy massage at the Yusupov Hospital is carried out by a senior exercise therapy instructor who has knowledge of the anatomy and physiology of muscles and the speech apparatus, has undergone special training, and is fluent in massage techniques.
Rehabilitation specialists teach those caring for a patient with dysarthria basic massage techniques and passive articulatory gymnastics. Differentiated speech therapy massage is necessary to normalize the muscle tone of the articulatory apparatus, and in more severe cases, to reduce the degree of manifestation of motor defects of the articulatory muscles:
- Hyperkinesis (excessive violent motor acts that occur against the will of the patient);
- Spastic paresis,
- Ataxia (impaired coordination of movements not associated with muscle weakness);
- Synkinesia (additional movements that occur involuntarily during basic functional movements).
With its help, they activate those muscle groups of the peripheral speech apparatus that cannot fully contract, or activate new muscle groups that were previously inactive, stimulate proprioceptive sensations, and reduce the secretion of saliva. Speech therapy massage strengthens the pharyngeal reflex, prepares conditions for the formation of voluntary, coordinated movements of the articulation organs.
The essence of speech therapy massage is the application of mechanical irritations:
- Stroking;
- Tingling;
- Kneading;
- Rubbing;
- Vibrations;
- Effleurage.
The differentiated use of various massage techniques allows rehabilitation specialists at the Yusupov Hospital to reduce muscle tone in case of muscle spasticity or increase it in case of hypotonia of the articulatory muscles. Subsequently, the patient develops and carries out voluntary (active), coordinated movements of the articulation organs. Speech therapy massage is performed in the area of the muscles of the head, neck, and upper shoulder girdle. Particular attention is paid to the muscles of the peripheral speech apparatus (tongue, lips, soft palate and cheeks), as they ensure the production of speech.
Stages of correction of sound pronunciation disorders
The speech therapist adheres to a strict sequence of sound production for dysarthria. Corrective work consists of 6 stages.
First: the specialist prepares the articulatory base for the production and pronunciation of palatal, sonorant, hissing and whistling sounds. When the baby masters some of them, the speech therapist moves on to working on them. It involves kinesthetic, auditory and visual control. Here is an example of a speech therapist’s instructions to a small patient: “Look in the mirror and repeat after me,” “Look in the mirror and do the exercise,” “Look at yourself in the mirror, stretch out your lips.” This feature of sound production gives good results.
This approach is necessary to reduce the apraxic disorders that accompany dysarthria. In general, the first stage is the foundation for the further development of sound pronunciation skills.
Second: the speech therapist determines the sequence of correction. He assesses which articulatory structure the patient has “mature”. Many children with motor and speech disorders are better at producing more complex sounds, such as hissing sounds. But the patient can master lighter whistling sounds, with which it is recommended to begin correction, later.
Third: the specialist stimulates or plays a certain sound. When staging, he uses classical techniques - staging by imitation, mechanical or mixed method.
Fourth: consolidation, or automation. This is the most difficult stage in all correctional work. It takes the most time. Often children master a sound and pronounce it in isolation, but make mistakes in speech. Therefore, after the production stage, the speech therapist focuses on working on isolated sound pronunciation, and then connects words with different syllable structures. Thus, the child pronounces the sound at the beginning, middle or end of words. Then the speech therapist connects sentences in which the sound being studied is concentrated.
The speech therapist selects lexical material individually. It must be appropriate for the baby’s age and capabilities, and also not include sounds that he cannot yet pronounce or distort.
Fifth: separation of delivered and oppositional sounds. First, the speech therapist suggests 2 syllables, then increases to 3. for example, sa - sha, sta - shta, etc. After this, he works on pairs of words with different syllable structures.
Sixth: developing communication skills. Another difficult stage. Often children communicate in a speech therapist’s office, but in front of other people and outside the office, the acquired speech skills are lost, and the child begins to speak “the old fashioned way.” In order to develop communication skills, the painstaking work of a speech therapist is necessary, but without the desire of the child himself, success cannot be achieved either.
The development of communication skills in dysarthria is facilitated by techniques such as memorizing rhymes, retelling or writing stories.
Correction of the pronunciation aspect of speech
The pronunciation side of speech includes sound pronunciation and prosody (intonation, melody, pause, stress, tempo, rhythm and timbre). The functioning of the pronunciation side of speech is closely related to articulatory motor skills and the phonemic side of speech. Pronunciation of sounds is the phonetic design of speech and at the same time a complex of speech motor skills by which it is determined.
Corrective work is based on the following principles:
- Connections of speech with other aspects of mental development. To implement it, correctional influence is carried out not only on speech activity, but also on non-speech processes, the patient’s personality as a whole;
- Systematic approach. The pronunciation side is considered as a system that includes a number of components. Corrective work is aimed at their development (development of articulatory motor skills, sound pronunciation, phonemic perception, prosody);
- The development principle involves analyzing the process of the occurrence of a defect. The immediate result of impaired sound pronunciation in patients with dysarthria is limited mobility of the speech organs. Difficulties in articulation cause pronunciation deficiencies, which can be expressed to varying degrees. One manifestation may be a consequence or cause of another. Corrective work is directed not only at the consequence of the violation - defects in sound pronunciation, but also at their root cause - violations of articulatory motor skills.
Correctional speech therapy work is carried out using various methods: practical, visual, verbal. Practical methods include imitative-performing, constructive and creative exercises, games and modeling. Visually - observation, examination of profiles, diagrams, showing a sample task and method of action. The main verbal methods are conversation, reading, story.
Gymnastics for making sounds
Finger games must be included in the correction program for dysarthria. They can be done at home with your parents. For example, these:
- Reading book “Finger Boy, Where Have You Been?” The child opens his palm and, for each line of the rhyme, touches each finger with his thumb - index, middle, ring and little fingers.
- "We depict animals." This is an analogue of the “Shadow Theatre”. The kid opens his palm, sticks his thumb up - imitates a dog. Raises and lowers the little finger - the dog barks. And if you press your ring and little fingers with your thumb to your palm, and raise your middle and index fingers up, you will get a bunny that moves its ears.
- Hand massage. The technique depends on the tone of the hands.
If you have spasticity, you need to relax: stroke your arms: from your fingertips up to your palms and to your shoulders. Then repeat the movement from top to bottom.
When hypotonicity occurs, muscles need to be strengthened. To do this, parents actively knead and rub their fingers and palms. Stimulating movements.
A set of articulation exercises
The exercise includes 5 exercises and can also be done at home.
“Horse” - clicking the tongue. This is a very useful and effective exercise. Not all children get it right away.
“Pancakes” - the baby opens his mouth slightly, spreads his tongue into a flat pancake.
“Snake” - the child imitates the sting of a snake - the tongue is just as sharp. Then he sticks it back and forth.
“Tube” - the baby tries to roll his tongue into a tube.
Another exercise is to try to reach the tip of your tongue to your nose and then to your chin.
A set of breathing exercises
Includes 2 exercises. Parents can easily do them with their baby at home.
"Racing" . Place two cotton balls on the table. The parent blows on one balloon, the child on the other. The one who moves his ball the greatest distance wins.
"Magic Breath" . Insert pieces of cotton wool into the baby's nostrils. The main thing is not deep! Ask him to exhale and at the same time hold the cotton wool - it should not fall out.
Another version of breathing exercises is according to A.N. Strelnikova. The essence of gymnastics is to take a sharp breath through your nose every second and do the exercises at the same time. The inhalation is noisy and strong, and the exhalation is natural, imperceptible.
There are several rules: with each inhalation, lower your shoulders and close your nostrils tightly, as if someone is pressing on them.
Gymnastics should be a joy, so you need to do it until the first signs of fatigue. There is no need to force your child if he does not want to study.
Gymnastics is designed for adults, so the duration of the lesson and the number of approaches is best agreed upon with a speech therapist.
We train to navigate in space
- “Whose traces?” . Pictures with traces of hands and feet are needed. The baby must determine which arm or leg is right and which is left.
- "Supermarket" . The parent asks the child to arrange the goods: “on the shelf”, “near the cash register”, “to the right of the cookies”, “under the counter”.
- Counting sticks. Can be replaced with matches. The parent makes some figure out of them, and the baby makes a similar one according to the image.
This complex can also be performed at home.
Methods for diagnosing dysarthria
Dysarthria is usually preceded by a primary neurological disease, such as cerebral palsy. Therefore, before starting classes with a speech therapist, you need to consult a neurologist. Only he can diagnose the disease.
Diagnosis includes electroencephalography, MRI of the brain, electroneurography or other examinations. After this, the neurologist refers the patient to a speech therapist. In turn, the specialist, based on speech therapy tests, will determine the form and degree of the speech disorder.
Classification of dysarthria
The neurological classification of dysarthria is based on the principle of localization and a syndromic approach. Taking into account the localization of damage to the speech-motor apparatus, the following are distinguished:
- bulbar dysarthria associated with damage to the nuclei of the cranial nerves (glossopharyngeal, sublingual, vagus, sometimes facial, trigeminal) in the medulla oblongata
- pseudobulbar dysarthria associated with damage to the corticonuclear pathways
- extrapyramidal (subcortical) dysarthria associated with damage to the subcortical nuclei of the brain
- cerebellar dysarthria associated with damage to the cerebellum and its pathways
- cortical dysarthria associated with focal lesions of the cerebral cortex.
Depending on the leading clinical syndrome, cerebral palsy may include spastic-rigid, spastic-paretic, spastic-hyperkinetic, spastic-atactic, ataxic-hyperkinetic dysarthria.
Speech therapy classification is based on the principle of speech intelligibility for others and includes 4 degrees of severity of dysarthria:
1st degree (erased dysarthria) – defects in sound pronunciation can only be identified by a speech therapist during a special examination.
Grade 2 defects in sound pronunciation are noticeable to others, but overall speech remains understandable.
3rd degree - understanding of the speech of a patient with dysarthria is available only to those close to him and partially to strangers.
4th degree speech is absent or incomprehensible even to the closest people (anarthria).
Complex treatment of the disease
Only an integrated approach gives good results. Here are the activities included in treatment:
- Speech therapy classes: development of fine motor skills of the hands, breathing, motor skills of the speech apparatus, voice (timbre, intonation, strength), training in correct sound pronunciation;
- Physiotherapeutic procedures: physical therapy, massage, acupressure, etc.;
- Drug treatment. Nootropic drugs are prescribed;
- Psychotherapy. This group includes sand therapy, play therapy, and isotherapy.
If parents notice speech impairments in time and seek help from doctors, the baby has every chance of getting rid of the disease. But provided that there are no pronounced lesions of the nervous system.
Speech therapy exercises for erased dysarthria
Office of psychological and pedagogical correction of Lebyazhinsky district
Design of materials for information stands:
Speech therapy exercises for erased dysarthria.
Prepared by speech therapist teacher: Mukhambetova F.B.
Akku village 2021, December
According to research by R.I. Martynova, children with a mild form of dysarthria lag behind in physical development significantly more than children with functional dyslalia. In children with an erased form of dysarthria in the speech system, neurological symptoms were identified: erased paresis, hyperkinesis, disorders of muscle tone in the articulatory and facial muscles. Neuropsychiatric disorders were significantly more detected in mild forms of dysarthria than in functional dyslalia. That. The work of a speech therapist with children with an erased form of dysarthria should not be limited to the production and correction of defective sounds, but should have a wider range of correction of the child’s speech as a whole.
The peculiarities of the content of speech therapy work with an erased form of dysarthria are reflected in the specifics of planning correctional work: an additional preparatory stage is introduced, which is necessary to normalize motor skills and the tone of the articulatory apparatus, and the development of prosody.
Having studied the methods of L.V. Lopatina, N.V. Serebryakova, L.A. Danilova, I.I. Ermakova, E.M. Mastyukova, E.F. Arkhipova, I selected and systematized practical material for all sections of the preparatory stage, taking into account the speech and non-speech symptoms of dysarthria.
1) Normalization of muscle tone of the articulatory apparatus - differentiated speech therapy massage (method by E.F. Arkhipova)
For children with hypertonicity and hyperkinesis, a relaxing massage is recommended. In such children, the face is frozen, the muscles are stiff, the muscles of the lips are stretched and pressed against the gums, the tongue is thick and shapeless, the tip of the tongue is not pronounced. Massage techniques: patting, tapping, light vibration, stroking for no more than 1.5 minutes. All movements go from the periphery to the center: from the temples to the center of the forehead, nose, middle of the lips.
For children with hypotension - a strengthening massage. In such children, the facial muscles are flabby and loose, the mouth is open, the lips are flaccid, the thin tongue lies at the bottom of the mouth. Techniques: deep rubbing, kneading, stroking with force for up to 3 minutes. All movements are from the center of the face to the sides: from the forehead to the temples, from the nose to the ears, from the middle of the lips to the corners, from the middle of the tongue to the tip.
2) Normalization of motor skills of the articulatory apparatus:
exercises for masticatory muscles (met. I.I. Ermakova)
- Open your mouth and close it.
- Move the lower jaw forward.
- Open your mouth and close it.
- Puff out your cheeks and relax.
- Open your mouth and close it.
- Lateral movements of the lower jaw.
- Open your mouth and close it.
- Pull your cheeks in and relax.
- Open your mouth and close it.
- Bite your upper lip with your lower teeth
- Open your mouth with your head thrown back, close your mouth with your head straight.
gymnastics for voluntary tension and movement of lips and cheeks (met. E.F. Arkhipova)
- Inflating both cheeks at the same time.
- Puffing out the cheeks alternately.
- Retraction of the cheeks into the oral cavity.
- The closed lips are pulled forward with a tube (proboscis) and then returned to their normal position.
- Grin: the lips are stretched to the sides, pressed tightly against the gums, both rows of teeth are exposed.
- Alternating grin-proboscis (smile-pipe).
- Retraction of the lips into the oral cavity with the jaws open.
- Lifting only the upper lip, exposing only the upper teeth.
- Retraction of the lower lip, exposing only the lower teeth.
- Alternately raising and lowering the upper and lower lips.
- Imitation of rinsing teeth.
- Lower lip under upper teeth.
- Upper lip under lower teeth.
- Alternating the two previous exercises.
- Lip vibration (horse snorting).
- As you exhale, hold the pencil with your lips.
passive gymnastics for the muscles of the tongue - creating positive kinesthesia in the muscles (met. O.V. Pravdina)
Passive gymnastics is a form of gymnastics when a child makes movements only with the help of mechanical action - under the pressure of an adult's hand. . Passive movement should be carried out in 3 stages: 1 - entering the position (pucker your lips), 2 - maintain the position, 3 - exiting the position. After several repetitions, an attempt is made to perform the same movement one or two more times without mechanical assistance, i.e. passive movement is translated first into passive-active, and then into voluntary, performed according to verbal instructions.
An approximate complex of passive gymnastics:
- The lips close passively and are held in this position. The child's attention is fixed on closed lips, then he is asked to blow through his lips, breaking their contact;
- Using the index finger of the left hand, lift the child’s upper lip, exposing the upper teeth; with the index finger of the right hand, raise the lower lip to the level of the upper incisors and ask the child to blow;
- The tongue is placed and held between the teeth;
- The tip of the tongue is pressed and held against the alveolar process, the child is asked to blow, breaking the contact;
- The child's head is thrown back somewhat, the back of the tongue is raised towards the hard palate, the child is asked to make coughing movements, fixing his attention on the sensations of the tongue and palate.
active articulatory gymnastics - improving the quality, accuracy, rhythm and duration of articulatory movements; An important section of articulatory gymnastics for dysarthrics is the development of more subtle and differentiated movements of the tongue, activation of its tip, delimitation of movements of the tongue and lower jaw.
An approximate set of static articulation exercises for dysarthrics. L.V. Lopatina, N.V. Serebryakova
- Open your mouth, hold it open while counting from 1 to 5-7, close it.
- Open your mouth slightly, push your lower jaw forward, hold it in this position for 5-7 seconds, return to its original position.
- Pull the lower lip down, hold it while counting from 1 to 5-7, return to its original state; - raise your upper lip, hold it while counting from 1 to 5-7, return to its original state.
- - stretch your lips into a smile, exposing the upper and lower incisors, hold the count from 1 to 5-7, return to their original state; - stretch only the right (left) corner in a smile, exposing the upper and lower incisors, hold it counting from 1 to 5-7, return to its original position.
- - raise the right one, then the left one in turn: the corner of the lip, while keeping the lips closed, hold the count from 1 to 5-7, return to its original state.
- - stick out the tip of your tongue, mash it with your lips, pronouncing the syllables pa-pa-pa-pa. After pronouncing the last syllable, he will leave his mouth slightly open, fixing his wide tongue and holding it in this position, counting from 1 to 5-7; - stick the tip of your tongue between your teeth, bite it with your teeth, pronouncing the syllables ta-ta-ta-ta. After pronouncing the last syllable, leave the mouth slightly open, fixing the wide tongue and holding it in this position, counting from 1 to 5-7, return to its original position.
- - place the tip of the tongue on the upper lip, fix this position and hold it counting from 1 to 5-7, return to its original state; - place the tip of the tongue under the upper lip, fix it in this position, hold it while counting from 1 to 5-7, return it to its original state; - press the tip of the tongue to the upper incisors, hold the given position counting from 1 to 5-7, return to its original state; - the movement of “licking” with the tip of the tongue from the upper lip into the oral cavity behind the upper incisors.
- – give the tip of the tongue a “bridge” (“slide”) position: press the tip of the tongue against the lower incisors, raise the middle part of the back of the tongue, press the lateral edges to the upper lateral teeth, hold the specified position of the tongue counting from 1 to 5-7, lower the tongue .
An approximate set of dynamic articulation exercises for dysarthrics. L.V. Lopatina, N.V. Serebryakova
- Stretch your lips into a smile, exposing the upper and lower incisors; Pull your lips forward like a tube.
- Stretch your lips into a smile with your incisors bared, and then stick out your tongue.
- Stretch your lips into a smile with your incisors bared, stick out your tongue, press it with your teeth.
- Raise the tip of your tongue onto your upper lip and lower it onto your lower lip (repeat this movement several times).
- Place the tip of your tongue under the upper lip, then under the lower lip (repeat this movement several times)
- Press the tip of your tongue behind the upper, then lower incisors (repeat this movement several times).
- Alternately make the tongue wide, then narrow.
- Lift your tongue up, place it between your teeth, and pull it back.
- Build a “bridge” (the tip of the tongue is pressed against the lower incisors, the front part of the back of the tongue is lowered, the front part is raised, forming a gap with the hard palate, the back part is lowered, the lateral edges of the tongue are raised and pressed against the upper lateral teeth), break it, then build it again and again break, etc.
- Alternately touch the protruding tip of your tongue to the right, then to the left corner of your lips.
- Raise the tip of your tongue to the upper lip, lower it to the lower lip, alternately touch the protruding tip of the tongue to the right, then to the left corner of the lips (repeat this movement several times).
3) Development of fine motor skills of the hands:
- massage and self-massage of fingers and hands;
- games with small objects: stringing beads, mosaics, small construction sets;
- finger gymnastics complexes;
- developing self-service skills: buttoning and unbuttoning buttons, tying shoes, using a fork and knife;
- classes with plasticine and scissors;
- preparing your hand for writing: coloring and shading pictures, tracing stencils, graphic dictations, working with copybooks;
A set of exercises for self-massage of hands and fingers.
1. Children use the pads of four fingers, which are placed at the base of the fingers on the back of the hand being massaged, and dotted movements back and forth, shifting the skin by about 1 cm, gradually moving them towards the wrist joint (“dotted” movement).
Iron
We'll smooth out the wrinkles with an iron, everything will be fine. Let's iron all the pants of the hare, hedgehog and bear.
2. Using the edge of their palm, children imitate “sawing” in all directions on the back of the hand (“straightforward” movement). The hand and forearm are placed on the table, the children are sitting.
Saw
Drank, drank, drank, drank! Cold winter has come. Let's get some wood for us quickly, let's light the stove and warm everyone up!
3. Rotational movements are made with the base of the hand towards the little finger.
Dough
We knead the dough, we knead the dough, We will bake pies with cabbage and mushrooms. — Should I treat you to some pies?
4. Self-massage of the hand from the palm side. The hand and forearm are placed on the table or on the knee, the children are sitting. Stroking.
Mother
Mom strokes her little son on the head, Her palm is so tender, Like a willow twig. - Grow up, dear son, Be kind, brave, honest, Gain intelligence and strength. And don't forget me!
5. Move the knuckles of your fingers clenched into a fist up and down and from right to left along the palm of the hand being massaged (“straight-line movement”).
Grater
Together we help mom, grate beets with a grater, together with mom we cook cabbage soup, - Look for something tastier!
6. The phalanges of the fingers clenched into a fist make a movement according to the “gimlet” principle in the palm of the massaged hand.
Drill
Dad takes the drill in his hands, And it buzzes, sings, As if a fidgety mouse is gnawing a hole in the wall!
7. Self-massage of fingers. The hand and forearm of the arm being massaged are located on the table, the children are sitting. With “pincers” formed by the bent index and middle fingers, a grasping movement is made for each word of the poetic text in the direction from the nail phalanges to the base of the fingers (“rectilinear” movement).
Ticks
The pliers grabbed the nail and tried to pull it out. Maybe something will work out if they try!
8. The pad of the thumb, placed on the back side of the massaged phalanx, moves, the other four cover and support the finger from below (“spiral” movement).
Lambs
“Byashki”, curly-haired lambs, graze in the meadows. All day long it’s all: “Be and be,” They wear fur coats on themselves. Fur coats in curls, look, “Byashki” slept in curlers, In the morning they took off the curlers, Try to find a smooth one. Everyone is curly-haired, every single one, They run in a curly-haired crowd. This is their fashion, the sheep people.
9. Movements as when rubbing frozen hands.
Morozko
Morozko froze us, crawled under a warm collar, like a thief, carefully penetrated into our felt boots. He has his own worries - Know the frost, but get stronger! Don’t spoil, Frost, why don’t you treat people like that?!
4) Development of general motor skills and motor coordination:
- pantomime (book “Tell Poems with Your Hands”, “Psychogymnastics” by M.I. Chistyakov, “Movement and Speech” by I.S. Lopukhin);
- outdoor games for coordination and coordination of movements;
- special complexes of physical and rhythmic exercises (journal “Defectology” No. 4, 1999)
5) Normalization of voice and speech breathing:
— Breathing exercises by A.N. Strelnikova.
— Exercises for the development of speech breathing
The following exercises are recommended in speech therapy practice:
- Choose a comfortable position (lying, sitting, standing), place one hand on your stomach, the other on the side of your lower chest. Take a deep breath through your nose (this pushes your stomach forward and expands your lower chest, which is controlled by both hands). After inhaling, immediately exhale freely and smoothly (the abdomen and lower chest return to their previous position).
— Take a short, calm breath in through your nose, hold the air in your lungs for 2-3 seconds, then exhale long, smoothly through your mouth.
— Take a short breath with your mouth open and, with a smooth, drawn-out exhalation, pronounce one of the vowel sounds (a, o, u, i, e, s).
- Smoothly pronounce several sounds on one exhalation: aaaaa aaaaaooooooo aaaaaauuuuuu
- Count on one exhalation up to 3-5 (one, two, three...), trying to gradually increase the count to 10-15. Make sure you exhale smoothly. Count down (ten, nine, eight...).
- Read proverbs, sayings, tongue twisters in one breath. Be sure to follow the instructions given in the first exercise.
Practiced skills can and should be consolidated and fully applied in practice.
The tasks become more complex gradually: first, long speech exhalation training is carried out on individual sounds, then on words, then on a short phrase, when reading poetry, etc.
In each exercise, children’s attention is directed to a calm, relaxed exhalation, to the duration and volume of the sounds pronounced.
“Skits without words” help normalize speech breathing and improve articulation in the initial period. At this time, the speech therapist shows the children an example of calm expressive speech, so at first he speaks more during classes. “Skits without words” contain elements of pantomime, and speech material is specially kept to a minimum in order to provide the basics of speech technique and eliminate incorrect speech. During these “performances” only interjections are used (Ah! Ah! Oh! etc.), onomatopoeia, individual words (names of people, names of animals), and later short sentences. Gradually, the speech material becomes more complex: short or long (but rhythmic) phrases appear as speech begins to improve. The attention of beginning artists is constantly drawn to what intonation should be used to pronounce the corresponding words, interjections, what gestures and facial expressions to use. During the work, children’s own imaginations are encouraged, their ability to choose new gestures, intonation, etc.
Also, for the development of proper speech breathing, the following are recommended:
- special exercise games: playing pipes, blowing away small objects, blowing soap bubbles, etc.
- phonetic rhythm by Mukhina A.Ya.;
- voice exercises by Ermakova I.I., Lopatina L.V.
6) Formation of the prosodic side of speech according to met. Lopatina L.V.:
- exercises to develop rhythm (perception and reproduction of rhythm);
- exercises to master the rhythm of words;
- familiarity with narrative, interrogative, exclamatory intonation;
- formation of intonation expressiveness in expressive speech
7) Overcoming sensory impairments:
- development of spatio-temporal concepts in met. Danilova L.A.
- exercises to develop the sense of touch in met. Danilova L.A.
System of classes for preschool children (from 5 to 7 years old)
Development of spatial concepts.
- Determination of basic spatial (prepositional) relations on specific objects. The child, according to the instructions, rearranges the objects in the indicated directions.
- The name of the main spatial relationships in the plot picture.
- Development of constructive praxis.
- Development of spatial relationships in a child’s visual activity.
- Memory training for spatial relationships. Analysis of a picture from memory, taking into account the spatial relationships between objects. A story from memory about the location of objects in space... Training of trace tests of constructive praxis.
Office for the Development of Touch.
- Training to determine the texture of an object. Recognition of texture by touch during preliminary display.
- Determination of the texture and shape of real objects without prior demonstration.
- Differentiation by touch of different geometric bodies: a) the same shape, but different thicknesses (flat and volumetric); b) the same shape and thickness, but different sizes (large and small); c) the same size and thickness, but different shapes... The development of this ability is formed in stages:
- Stage I - recognition of three-dimensional figures by touch after preliminary visual familiarization with the figure;
- // stage - recognition of three-dimensional figures of the same texture without preliminary display;
- Stage III - recognition of flat figures of the same texture after visual familiarization;
- Stage IV - recognition of flat figures by touch without display;
- Stage V - recognition of figures by touch of the same shape, but different in texture after their preliminary examination;
- Stage VI - recognition of the shape and texture of an object by touch without prior inspection;
- Stage VII - distinguishing objects of the same shape and texture by size by touch...
 Development of temporal representations.
Development of temporal representations.
- Determination of the sequence of seasons, clarification in pictures and in verbal descriptions of the distinctive features of each season.
- Sequence of periods of the day, analysis of regime moments.
- Practicing the concepts of “older - younger”.
To form generalizations, exercises are carried out to develop generalizations by the method of elimination (the game “The Fourth Extra”).
- / stage - 4 objects are laid out in front of the child, united by certain properties.
- // stage - eliminating unnecessary objects in the picture.
To develop an understanding of cause-and-effect relationships
a guessing game is used... During the game, independent observations and certain concepts about objects are formed, cause-and-effect relationships are revealed.
As many years of observations have shown, the proposed correction methods can significantly develop unformed functions and prepare the child to perceive
9) Development of phonemic hearing according to met. T.A. Tkachenko, L.V. Lopatina, N.V. Serebryakova
Speech therapy work for erased forms of dysarthria at the preparatory stage ensures the effectiveness of correction at all subsequent stages of correctional work.
Methods for preventing the disease
Due to the biological factors in the development of the disease, it is worth thinking about its prevention during pregnancy and childbirth. Difficult pregnancy, intrauterine infections, asphyxia, complicated childbirth, injuries in the first months of a newborn’s life - all this can cause speech disorders in the future.
We list the main methods of preventing the disease after the birth of the baby.
First, develop your reflexes. These include gaze fixation and object tracking, auditory concentration, motor activity, and the oral automatism reflex - all of them are very important in the development of the newborn.
Secondly, communicate with the baby. Tactile, visual, auditory sensations - all this is extremely important for its development. Smile at him, talk to him, carry him in your arms, stroke him.
Third, be always there. This is especially true for mom. After all, a newborn needs her closeness, the opportunity to touch her, see her, feel her, and receive a return hug.
Fourth, stimulate the sucking reflex. The more actively and longer the baby suckles at the breast, the better its muscles develop - they become stronger and more flexible.
Fifth, encourage the baby's attempts to communicate. Humming and babbling - this needs to be stimulated.
Sixth, develop fine motor skills. Speech is directly related to fine motor skills and the more dexterous the baby’s hands are, the better. Introduce him to different textures.
Seventh, speak to your baby in your native language. Speak clearly and competently. And encourage him to communicate. Even if he doesn't talk, still try to make him make sounds. If he wants something and shows it with gestures, provoke him to ask for it verbally.
Characteristics of clinical forms of dysarthria
Bulbar dysarthria is characterized by areflexia, amymia, disorder of sucking, swallowing solid and liquid food, chewing, hypersalivation caused by atony of the muscles of the oral cavity. The articulation of sounds is slurred and extremely simplified. All the variety of consonants is reduced into a single fricative sound; sounds are not differentiated from each other. Nasalization of voice timbre, dysphonia or aphonia is typical.
With pseudobulbar dysarthria, the nature of the disorder is determined by spastic paralysis and muscle hypertonicity. Pseudobulbar paralysis manifests itself most clearly in impaired tongue movements: great difficulty is caused by attempts to raise the tip of the tongue upward, move it to the sides, or hold it in a certain position. With pseudobulbar dysarthria, switching from one articulatory posture to another is difficult. Typically selective impairment of voluntary movements, synkinesis (conjugal movements); profuse salivation, increased pharyngeal reflex, choking, dysphagia. The speech of patients with pseudobulbar dysarthria is blurred, slurred, and has a nasal tint; the normative reproduction of sonors, whistling and hissing, is grossly violated.
Subcortical dysarthria is characterized by the presence of hyperkinesis - involuntary violent muscle movements, including facial and articulatory movements. Hyperkinesis can occur at rest, but usually intensifies when attempting to speak, causing articulatory spasm. There is a violation of the timbre and strength of the voice, the prosodic aspect of speech; Sometimes patients emit involuntary guttural screams.
With subcortical dysarthria, the tempo of speech may be disrupted, such as bradylalia, tachylalia, or speech dysrhythmia (organic stuttering). Subcortical dysarthria is often combined with pseudobulbar, bulbar and cerebellar forms.
A typical manifestation of cerebellar dysarthria is a violation of the coordination of the speech process, which results in tremor of the tongue, jerky, scanned speech, and occasional cries. Speech is slow and slurred; The pronunciation of front-lingual and labial sounds is most affected. With cerebellar dysarthria, ataxia is observed (unsteadiness of gait, imbalance, clumsiness of movements).
Cortical dysarthria in its speech manifestations resembles motor aphasia and is characterized by a violation of voluntary articulatory motor skills. There are no disorders of speech breathing, voice, or prosody in cortical dysarthria. Taking into account the localization of lesions, kinesthetic postcentral cortical dysarthria (afferent cortical dysarthria) and kinetic premotor cortical dysarthria (efferent cortical dysarthria) are distinguished. However, with cortical dysarthria there is only articulatory apraxia, while with motor aphasia not only the articulation of sounds suffers, but also reading, writing, understanding speech, and using language.
conclusions
Dysarthria is not just a failure to pronounce certain sounds. And you certainly shouldn’t expect a child with such a diagnosis to “talk” like the neighbors’ daughter. This speech disorder is much deeper and more complex, but it is not always a death sentence. The main thing is not to waste time.
This is why turning a blind eye to the problem is a huge mistake as parents. Of course, it is difficult to accept the fact that your child has some kind of impairment. But this must be done precisely for the benefit of the future of your baby. An untreated disease will bring many problems to an adult in social life - from communication to work.
If the disease is detected at an early stage of development, it can be cured. An integrated approach to therapy gives good results. Of course, if there are no gross disorders of the nervous system.
It is even better if it was possible to diagnose the disease when it has not yet made itself felt, that is, before the baby’s first attempts to speak. Such early corrective work will become effective prevention.