Methodology for screening examination of patients with aphasia
The invention relates to the field of medicine and pedagogy, namely to neurology and speech therapy. It can be used in neurological and neurosurgical clinics, in rehabilitation departments for patients with organic brain damage. A distinctive feature of the proposed diagnostic method is that the examination of the patient consists of several independent modules, which are grouped in accordance with the diagnosed forms of aphasia. In each module, a specific form is tested and the degree of its expression is determined.
Key words: screening examination methodology, aphasia, forms of aphasia
Currently, significant progress has been made in medicine [5–22], including the treatment of aphasia. The pathogenesis of aphasia is characterized by a systemic impairment of the functioning of speech thinking due to organic damage to the brain.
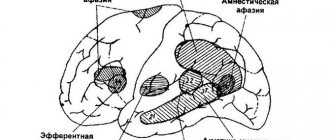
Aphasia is clinically manifested:
1) in a gross violation of understanding and one’s own speech (severe sensorimotor aphasia);
2) in violation of the understanding of addressed speech (acoustic-gnostic aphasia);
3) in violation of the volume of auditory-verbal memory (acoustic-mnestic aphasia);
4) in violation of the semantics of speech (semantic aphasia);
5) in violation of the motor kinesthetic program (afferent-motor aphasia);
6) in violation of the motor kinetic program (efferent-motor aphasia);
7) in violation of planning and programming of speech utterance (dynamic aphasia).
Mutism, that is, a voluntary refusal of verbal communication that is not caused by organic changes in the cerebral cortex, should be differentiated from aphasia syndrome. The essence of this work was the consistent arrangement and integration of material on the diagnosis of people with aphasia until the final examination methodology was obtained. When assembling information, the structural components of the diagnosis (preconditions and manifestations) were determined by comparing different manifestations to specific symptoms or syndromes. In this case, a qualitative analysis of the defect was used, identifying the primarily affected links (factors). This made it possible to distinguish similar patterns of disturbance and contributed to the formulation of an accurate speech therapy diagnosis. In general, the process of creating a computer express examination technique consisted of several stages:
- grouping existing symptoms into a syndrome;
- identification of the leading symptom in the syndrome;
- recognition of the resulting syndrome by comparison with standard ideas about the forms of aphasia.
When examining a patient, personal data, clinical diagnosis, characteristics of the patient’s emotional-volitional sphere, and the results of objective studies (CT/MRI) are initially recorded. At the next stage, the actual study of the patient’s speech thinking begins, which consists of two stages. The goal of the first stage is to exclude the gross severity of the speech disorder, as well as to differentiate aphasia and mutism. The purpose of the second stage is to determine the form of aphasia and the degree of its severity.
The result of the examination is a score that correlates with the form of speech impairment and the degree of its severity. The screening methodology for examining patients with aphasia is based on proven, tested methods used in clinics to determine the detection of speech disorders in patients with local cerebrovascular accident [1,2,3,4,5,6].
The creation of a computer screening diagnostic technique was carried out in 2013–2015. in several stages: At the first stage, the developer (speech therapist M.M. Shcherbakova), based on the analyzed literature and his own implemented rehabilitation programs, compiled an express method for diagnosing aphasia that meets all the requirements for these works. He controlled the process, analyzed the content of the express method and its adequacy of application in the clinic, the head of the neurology department, the chief freelance specialist of the Moscow Region, the head of the department of neurology of the Federal Institution of Healthcare of the Moscow Region MONIKI named after. M. V. Vladimirsky, Doctor of Medical Sciences, Professor S. V. Kotov. At the second stage, a computer version of express diagnostics was created (programmers from the computer technology department of the Federal University of Internal Affairs of the State Budgetary Institution of Healthcare of the Moscow Region MONIKI named after M. F. Vladimirsky MONIKI.). At the third stage, computer screening diagnostics of aphasia was tested in the clinic (department of neurology of the Federal State Budgetary Institution of Healthcare of the Moscow Regional Research Institute named after M. F. Vladimirsky) and proved its reliability.
The examination algorithm is simple and accessible to specialists, since: 1) it does not require additional materials; 2) is available for examination of patients by both speech therapists-aphasiologists and neurologists. The duration of the examination of one patient ranges from 7 to 30 minutes and does not require much mental stress from the patient.
The method is carried out as follows. Initially, general information about the patient, neurological diagnosis, disability group, education of the patient, features of the emotional-volitional sphere of the patient are recorded, the presence or absence of focal brain damage is clarified according to objective studies (CT/MRI). Then the actual process of examining the patient’s speech thinking begins, which consists of several independent modules. A change of instruction (movement to the next task) occurs when the last element in the proposed task is selected, or after the time allotted for completing the task has expired.
Module 1. Examination of gross sensorimotor aphasia. Includes 4 tasks. Assignments: situational conversation (3 points); automated speech (2 points); negotiation of persistent speech structures (3 points); understanding of simple verbal instructions (4 points).
Examination result:
1) 0–6 points - total aphasia. Recommended Module 2. Elimination of mutism.
2) 7–9 points - severe sensorimotor aphasia.
3) 10–12 points - no gross sensorimotor aphasia. Further examination of the patient is recommended.
Module 2. Elimination of mutism. Includes 3 tasks and one additional one. Tasks: adding missing words to the text (1 point); display of object pictures according to instructions (1 point); completing sentences (4 points).
Examination result:
1) 0–2 points – no mutism. A diagnosis is made: total aphasia
2) 3 points - additional examination is carried out to exclude mutism. As a result of the examination: a) 0 points - mutism is excluded, gross sensorimotor aphasia is diagnosed; b) 1 point - mutism is confirmed.
3) 4–6 points – mutism.
Module 3. Acoustic-gnostic aphasia. Includes 6 tasks. Tasks: showing story pictures (4 points); display of object pictures (4 points); laying out captions for subject pictures (4 points); phonemic awareness (6 points); making words from letters (4 points).
Examination result:
1) 20–22 points - no acoustic-gnostic aphasia.
2) 16–19 points – mild acoustic-gnostic aphasia
3) 13–15 points—acoustic-gnostic aphasia of moderate severity.
4) 0–12 points—acoustic-gnostic aphasia of severe severity.
Module 4. Acoustic-mnestic aphasia. Includes 5 tasks. Tasks: showing half-drawn subject pictures (4 points); explanation of the functional purposes of objects (5 points); selection of analogy (2 points); auditory-verbal memory for a series of words (2 points), auditory-verbal memory for a text (4 points).
Examination result:
1) 16–17 points - no acoustic-mnestic aphasia.
2) 13–15 points – mild acoustic-mnestic aphasia
3) 7-12 points - acoustic-mnestic aphasia of moderate severity.
4) 0–6 points - acoustic-mnestic aphasia of severe severity.
Module 5. Semantic aphasia. Includes 7 tasks. Tasks: visual perception of proportions (1 point); perception of superimposed images (3 points); body diagram (4 points); determining the time on a clock (2 points); counting operations (1 point); understanding the figurative meaning of the word (4 points); understanding of logical and grammatical phrases (2 points).
Examination result:
1) 16–17 points - no semantic aphasia.
2) 14–15 points – mild semantic aphasia
3) 8–13 points—semantic aphasia of moderate severity.
4) 0–7 points – semantic aphasia of severe severity.
Module 6. Dynamic aphasia. Includes 5 tasks. Assignments: dynamic praxis (1 point); selection of synonyms for verb words (4 points), antonyms (4 points); constructing a phrase (sentence) (3 points); solving logical problems (3 points).
Examination result:
1) 14–15 points - no dynamic aphasia.
2) 12–13 points – mild dynamic aphasia
3) 8-11 points - dynamic aphasia of moderate severity.
4) 0–7 points - dynamic aphasia of severe severity.
Module 7. Efferent-motor aphasia. Includes 4 tasks. Tasks: reproduction of non-automated series (2 points); graphic praxis (2 points); composing words from syllables (4 points); composing words from letters with a known first letter (4 points).
Examination result:
1) 10–11 points - no efferent-motor aphasia.
2) 8–9 points - efferent-motor aphasia of mild severity
3) 5–7 points – efferent-motor aphasia of moderate severity.
4) 0–4 points - efferent-motor aphasia of severe severity.
Module 8. Afferent-motor aphasia. Includes 6 tasks. Assignments: automated writing (1 point); adding the first syllables to a word (4 points); adding the last syllables to a word (4 points); making words from letters (3 points); guessing a crossword puzzle (5 points); disautomated writing (2 points).
Examination result:
1) 18–19 points - no afferent-motor aphasia.
2) 14–17 points – mild afferent-motor aphasia
3) 7–13 points - afferent-motor aphasia of moderate severity.
4) 0–6 points - afferent-motor aphasia of severe severity.
Thus, diagnosing a patient’s speech thinking using a unique method includes either:
1) all examination modules with determination of the form of aphasia and the degree of its severity in patients without a preliminary diagnosis. The procedure takes about 30 minutes.
2) a certain examination module in patients with a preliminary diagnosis in order to confirm the presence of this form of aphasia and determine the degree of its severity. The examination procedure takes 5–7 minutes.
The technique was tested in the neurological department of the State Budgetary Institution of Healthcare of the Moscow Region MONIKI named after. M. F. Vladimirsky in 2013–2015 for 137 patients. In most cases, patients had combined speech diagnoses. All examined patients (137 people) were given a preliminary speech therapy diagnosis, which was confirmed in 100% of cases when examined using a screening examination method. After the course of rehabilitation, the patients were re-examined using the screening examination method, which made it possible to prove the effectiveness of complex treatment (vascular therapy and speech therapy). If no speech disorders were identified during the initial examination, a repeat examination was not performed.
In general, the following advantages of computer screening methods for examining patients with aphasia can be noted:
1) the diagnostic methodology takes into account all parameters of the manifestation of aphasia syndrome (impairment of both speech and non-speech higher mental functions).
2) the examination algorithm is simple and accessible to specialists, since:
a) does not require additional materials;
b) is available for examination of patients by both speech therapists-aphasiologists and neurologists working with this group of patients.
3) the duration of examination of one patient ranges from 7 to 30 minutes and does not require much mental stress from the patient.
Literature:
- Ananyeva N.I., Kruglov L.S. et al. Complex diagnosis of vascular dementia. A manual for doctors, - Publishing house of the St. Petersburg Scientific Research Psychoneurological Institute named after. V. M. Bekhtereva, 2007
- Akhutina T.V., Tsvetkova L.S., Pylaeva N.M. Methodology for assessing speech in aphasia - M. Moscow State University Publishing House 1981
- Vaserman L. I., Dorofeeva S. A., Meerson Ya. A. Methods of neuropsychological diagnostics - St. Petersburg, 1997
- Common scales in neurology - Collection "NPK PHARMASOFT" 2012
- Shklovsky V. M. Card of neuropsychological research of patients with disorders of higher mental functions - M. Department of Speech Pathology, Moscow Research Institute of Psychiatry, Ministry of Health of the RSFSR, 1996
- Benton, Hamsher Multilingual Aphasia Examination, 1989
- Molochkov A.V., Kildyushevsky A.V., Karzanov O.V., Bagapsh L.S. Clinical effectiveness of extracorporeal photochemotherapy for lupus erythematosus. // Almanac of Clinical Medicine. 2014. No. 34. pp. 15–19
- Molochkov V. A. Treatment of psoriasis with homeopathic medicines // Almanac of Clinical Medicine. 2014. No. 34. pp. 20–25
- Molochkov A. V., Romanko Yu. S., Kazantseva K. V., Sukhova T. E., Popuchiev V. V., Tretyakova E. I., Matveeva O. V., Kuntsevich Zh. S., Molochkova Yu V. et al. Laser-induced thermotherapy and photodynamic therapy in dermatology: possibilities and prospects. // Almanac of Clinical Medicine. 2014. No. 34. pp. 30–35
- Molochkov V. A., Kuntsevich Zh. S., Bobrov M. A. et al. Eruptive keratoacanthoma of the Grzebowski type. // Almanac of Clinical Medicine. 2014. No. 34. pp. 36–41
- Molochkov V. A., Korneva L. V., Snarskaya E. S., Shcherbakova E. O., Polyanskaya A. A., Nodelman E. K. Association of benign epithelial neoplasia with human papillomavirus beta. // Almanac of Clinical Medicine. 2014. No. 34. pp. 47–51
- Molochkov V. A., Korneva L. V., Snarskaya E. S., Shcherbakova E. O., Polyanskaya A. A., Trofimova O. B. Comparative analysis of the association of seborrheic keratosis with human papillomavirus in immunosuppressed and immunocompetent patients. // Almanac of Clinical Medicine. 2014. No. 34. P.52–55
- Molochkov A.V., Khlebnikova A.N. Possibilities of liposomal cosmetics acid in the treatment of chronic dermatoses (literature review). // Almanac of Clinical Medicine. 2014. No. 34. pp. 85–90
- Molochkov V. A. et al. Indinol forto and egallochite in the treatment of genital and giant condylomas. // Almanac of Clinical Medicine. 2014. No. 34. P. 100–105
- Molochkov V. A. Sildenafil and chronic prostatitis. // Almanac of Clinical Medicine. 2014. No. 34. pp. 108–111
- Glazkov A. A., Kulikov D. A., Dreval A. V. et al. Development of a method for diagnosing blood microcirculation disorders in patients with diabetes mellitus using laser Doppler flowmetry. // Almanac of Clinical Medicine. 2014. No. 31. P. 7–10
- Kulikova P. A., Filyushkin Yu. N., Kulikov D. A., Fedulov A. V., Mashkov A. E., Kulikov A. V. Experimental model of primary male hypogonadism. // Almanac of Clinical Medicine. 2014. No. 31. P.21–24
- Shcherbakova M. M. et al. Rehabilitation of patients with aphasia using modified recovery methods. // Almanac of Clinical Medicine. 2014. No. 31. P.56–60
- Molochkov A.V., Kildyushevsky A.V., Karzanov O.V., Bagapsh L.S. Clinical effectiveness of extracorporeal photochemotherapy for lupus erythematosus. // Almanac of Clinical Medicine. 2014. No. 34. pp. 15–19
- Dmitrieva N. G., Yakovchik O. N., Vatazin A. V. et al. Histocompatibility system for kidney transplantation. // Almanac of Clinical Medicine. 2014. No. 31. P.83–87
- Rudenko T. E., Kutyrina I. M., Shvetsov M. Yu., Androsova S. O. Stiffness of the common carotid and femoral arteries at the predialysis stage of chronic kidney disease. // Almanac of Clinical Medicine. 2014. No. 30. P. 25–31
- Gordovskaya N. B., Korotchaeva Yu. V. Asymptomatic bacteriuria in pregnant women: diagnosis and treatment. // Almanac of Clinical Medicine. 2014. No. 30. P.57–60
Treatment of aphasia
Treatment of aphasia requires a comprehensive approach. To correct the disease, drug therapy, surgery, and rehabilitation procedures are prescribed.
Medicines are selected individually depending on the causes of aphasia. Operations are carried out strictly according to indications. Rehabilitation procedures include massage, physiotherapy, acupuncture, mechanotherapy and exercise therapy.
During treatment, patients are under the supervision of a neurologist, neurosurgeon, and speech therapist.