Neurologist
SEMENOVA
Olga
5 years experience
neurologist, head of the office for diagnostics and treatment of cognitive disorders
Make an appointment
Aphasia is a speech disorder associated with dysfunction of the corresponding part of the cerebral cortex. Unlike dysarthria, this pathology is not associated with poor pronunciation of words and sounds. It does not allow the patient to fully form his own speech and perceive the words addressed to him. Typically, aphasia is a nonspecific sign of brain diseases - from circulatory disorders to the consequences of traumatic cell damage, etc.
What is amnestic aphasia?
Aphasia is a neurological disease of organic nature, which is formed as a result of the death of neurons located in the cerebral cortex area, responsible for the synthesis and formation of speech function, as well as the perception of speech and non-verbal signals of surrounding people. Aphasia is always an acquired pathology, i.e. it is observed in people with initially normally functioning speech function, so it is important not to confuse aphasia with alalia if the disease is observed in childhood.
A wide range of reasons can lead to the development of pathology, but the final pathogenetic mechanism of this disease is the same and consists in extensive death of nervous tissue localized in specific areas of the brain responsible for speech.
Amnestic-semantic aphasia and other types
In the Russian Federation, the classification of the Soviet neurologist A.R. is used. Luria. He divided aphasia into several types for the purpose of more convenient diagnostic testing for this pathology. Luria identified the following types of aphasia:
- Efferent motor. It occurs as a result of traumatic damage and dysfunction of the speech center located in the temporal lobes of the cerebral cortex. The victim has difficulty perceiving information when reading and writing: efferent motor aphasia is characterized by both spelling and punctuation errors, and problems also arise when moving from one thought process associated with speech synthesis to another.
- Afferent motor. In this case, the problem is associated with dysfunction of the central and parietal parts of the cerebral cortex. The patient has difficulty pronouncing words that are similar in phonetic and articulatory parameters. It is very difficult for such patients to find the necessary sound, which distorts their spoken speech.
- Acoustic-mnestic. Occurs when there is a defect in neural axonal and dendritic connections between the auditory analyzer and the hippocampal structures of the deeper subcortical parts of the brain. Such aphasia is manifested by impoverishment of speech, omission of parts of speech, and the presence of paraphrased speech errors.
- Dynamic aphasia. The cause may be a defect in the cortex, which is responsible for the motor center of speech function. Such people have problems constructing sentences, the logic and sequence of the spoken phrase or sentence is disrupted.
- Sensory aphasia is associated with a disorder of phonemic hearing, i.e. the patient does not logically perceive someone else's speech. This type of aphasia can be compared with the perception of a foreign language when you do not know it.
- Semantic aphasia. It is manifested by a lack of awareness and analysis of complex grammatical structures in a sentence; a person is able to understand only short phrases.
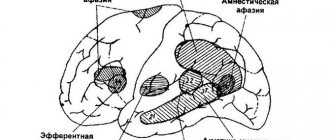
- Amnestic aphasia. Characterized by disruption of the parietal and temporal areas of the cerebral cortex. A form of the disease associated with a disruption of the innervation between a visible object and its verbal interpretation when reproducing this object. In such situations, the injured person understands what object is in front of him and can describe it, but cannot accurately name it. The speech of such a person becomes fluent, fussy, the patient tries to select many words, but they are inaccurate in meaning and objective characteristics. There is a feeling that the person has forgotten the name of the object. Very often combined with other forms, such as amnestic-semantic aphasia and sensory-amnestic aphasia.
- There is also a subtype of amnestic aphasia: optical-mnestic aphasia. Damage to the temporal cortex. The main problem is the inaccuracy of visual images of words; patients try to describe the function of an object, but cannot name it. Despite good orientation in space and time, patients have a pronounced defect in the image of objects - for example, they can copy a picture, but are not able to independently draw the picture from memory or following instructions. Also, such patients have impairments in written speech: in severe cases, patients cannot see the text on the left side.
Causes
Amnestic aphasia is usually observed when the white matter is damaged at the junction of the parietal, occipital and temporal parts of the left or right hemisphere of the brain. It is important to note that the disease does not appear on the affected side, but on the opposite side. In left-handers, the right hemisphere is damaged, and in right-handers, the left. The main etiological reasons are the following factors:
- Traumatic damage to the above-described areas of the brain. Most often this occurs during road traffic accidents and blunt blows to the temporal region of the head with a heavy object. In this case, a rupture of axonal connections of the white matter of the brain of a traumatic nature may form.
- Surgical interventions on brain structures. Damage to neighboring brain structures cannot be ruled out, since anatomically all zones and regions of the brain are closely connected.
- Infectious and inflammatory diseases such as meningitis, encephalitis and brain abscess. Infectious diseases can be of viral or bacterial etiology and often lead to generalized brain damage.
- Neoplasms of a benign or malignant nature.
- Acute and chronic cerebrovascular accidents causing stroke, thrombosis of cerebral vessels or discirculatory encephalopathy.
- Acute intoxication of the body, especially with neurotoxic poisons, or as a result of an overdose of certain medications.
- Separately, lesions of nervous tissue are distinguished in acute renal or liver failure. In this form, metabolic and breakdown products are not removed from the body in a timely manner and lead first to dysfunctional disorders and then to organic damage to brain tissue.
- Mental illnesses.
- Alzheimer's disease and Pick's disease. In Alzheimer's disease, a combination of sensory aphasia with amnestic aphasia is often characteristic, and in Pick's disease, a combination with motor aphasia is more often observed.
There are several risk groups for amnestic aphasia:
- Genetic predisposition. If there are relatives in the family with similar diseases, then the hereditary history is burdened and significantly increases the risk of aphasia for the reasons described above.
- Elderly and senile age. Common extragenital diseases: coronary heart disease, hypertension, epileptic seizures or cluster headache.
How to prevent the development of the disease
Prevention of amnestic aphasia is based on preventive measures that cause damage to the structures of the central nervous system. This includes the following medical recommendations:
- avoid situations that can lead to traumatic brain injuries (use a helmet and other protective equipment when engaging in hazardous sports);
- if you have a disease of the cardiovascular system or other internal organs, follow the doctor’s instructions and do not self-medicate;
- after neurosurgical operations, undergo full rehabilitation measures aimed at restoring cognitive skills;
- regularly engage in sports, including aerobic exercise and strength training;
- eliminate bad habits - drinking alcohol and smoking;
- normalize the diet by excluding from it all fatty, salty, smoked foods, and increasing the proportion of lean meats (chicken, rabbit), fish, fruits, vegetables and berries;
- in old age, continue to read books, learn poetry, do handicrafts and other hobbies (such activities prevent the development of Alzheimer's disease and Pick's disease).
If you detect any signs of amnestic aphasia in yourself or a close relative, you should immediately seek medical help. The pathology is treated by a neurologist or psychiatrist. In the absence of these specialists, it is necessary to visit a therapist who will conduct an initial diagnosis and refer the patient for further consultation to specialized medical institutions.
The prognosis depends on the degree of damage to the nerve tissue and the time of initiation of treatment and rehabilitation. With a small affected area and early initiation of therapy, the patient gradually recovers normal speech and other cognitive skills. If treatment is started late, its effectiveness is limited. Residual speech defects of varying severity are possible. The support of loved ones who are directly involved in the rehabilitation of the patient is important in eliminating aphasia.
Symptoms and manifestations
Amnestic aphasia is characterized by a mild course of the disease and a blurred manifestation of the clinical manifestations of the disease. Among the most common manifestations are the following symptoms:
- Slow speech of the victim, with pronounced intervals between sentences, or vice versa, the victim’s speech becomes fluent, illogical, turning into “porridge”;
- Repeated repetition of the same words or phrases;
- The presence of paraphrases is a descriptive characteristic of the semantic load of a word. Speech becomes descriptive;
- The patient misses words, most often nouns;
- Also, the patient cannot remember the name of the item or object in question, but knows its function and appearance.
Despite this, the patient's reading and writing skills do not suffer. His speech is constructed correctly, both grammatically and logically. The patient does not have difficulties with the acoustic pronunciation of words, as well as articulation. The patient's speech becomes expressive and replete with a large number of verbs.
It is important to note that the patient easily remembers the name of an object when prompted or in context, for example, if you name the first syllable of the desired word, the patient will easily remember its ending.
Diagnostics
Amnestic aphasia is a disease that lies at the intersection of two areas: neurology and psychology. Since aphasia is characterized by various disorders of the cognitive function of the brain, such disorders cannot but be accompanied by mental defects. Neuropsychological diagnostic methods are used to identify amnestic aphasia. To verify the disease and clarify the degree of impairment of the functional activity of the speech apparatus of a sick person, they resort to the use of special tests. Typically, such tests use a variety of objects with varying degrees of difficulty in pronouncing their names. There are also tests of a descriptive nature, when the patient is told about the characteristics of an object and see if the patient can answer with hints. A number of tests determine the connection between speech and visual manifestations, for example, the patient is sequentially shown several objects belonging to the same category; if the patient does not respond, then he has a violation of the connection between speech function and visual images, which can be interpreted in favor of sensory-amnestic aphasia.
In addition to special neurological and psychological tests, each patient is required to undergo laboratory and instrumental research methods. Depending on the cause of aphasia, diagnostic methods will be more or less informative.
The Clinical Brain Institute has a high-tech diagnostic department, which can conduct research such as:
- Tomographic studies: computed tomography and magnetic resonance imaging with and without contrast;
- X-ray examination of the skull and brain to identify defects;
- Ultrasound sonography and Doppler mapping of neck vessels;
- Comprehensive laboratory diagnostics.
In addition to high-quality equipment, a specialist is no less important for diagnostic purposes. The diagnostic department employs highly qualified specialists certified in related fields of medicine, which increases the efficiency of the diagnostic search and subsequent treatment of each individual patient.
Diagnostic measures
Diagnostics and treatment are handled by two specialists - a psychiatrist and a neurologist. Under no circumstances should you make a diagnosis or select therapy on your own. This can cause rapid progression of the underlying disease and the development of its complications. In medical institutions, the patient is examined according to the following algorithm:
- The patient's complaints, as well as anamnesis of life and illness, are collected. The specialist identifies factors and possible causes of brain damage. In most cases, it is necessary to additionally talk with loved ones.
- General clinical examinations: general and biochemical blood tests, general urinalysis, electrocardiogram, etc.
- Due to the presence of cognitive impairment, all patients are prescribed neuropsychological diagnostics based on the study of memory, attention, ability to perceive information, etc. Such methods make it possible to clarify the nature of the speech disorder, as well as to suggest the localization of the lesion in the brain.
- Computed or magnetic resonance imaging is used to study the structures of the central nervous system. The doctor has the opportunity to assess their integrity and identify areas of damage to the nervous tissue.
- If a traumatic brain injury is suspected, an X-ray examination of the skull is performed. The method allows you to identify damage to bone structures that indicate a head injury.
- In the case of neuroinfections, an enzyme-linked immunosorbent assay (ELISA) or polymerase chain reaction (PCR) of the patient’s blood and cerebrospinal fluid is performed to identify the pathogenic microorganism.
- Ultrasound and Doppler mapping of the cervical and cerebral vessels are used if symptoms are suspected of being ischemic. During the examination, the doctor can determine narrowing of the arteries, the formation of aneurysms, malformations, etc.
An integrated approach to diagnostics allows us to determine the exact location of brain damage and make an accurate diagnosis.
Treatment
Treatment of amnestic-semantic aphasia must be comprehensive. In this case, one should not hesitate, since the sooner corrective measures are started, the greater the patient’s chances of restoring lost cognitive functions.
After a diagnostic examination and clarification of the severity of damage to the speech centers of the brain, specialists formulate an individual treatment plan. In drawing up a treatment plan, in addition to functional and organic disorders, the patient’s age and mental state play an important role. Both a neurologist and a psychotherapist must work with each patient to achieve maximum effectiveness from therapy. If a serious organic pathology is detected that requires immediate surgical treatment, for example, in case of brain injuries or tumor lesions, emergency or planned surgical intervention is performed to eliminate the life-threatening condition and minimize cognitive impairment in the future.
Rehabilitation activities
Correct and comprehensive rehabilitation is of greatest importance in the correction of amnestic aphasia. Training aimed at restoring speech and other skills takes place in several stages:
- First, the patient is taught to work with objects through their visual image. To do this, use cards with an image and its name. This allows you to associate a certain visual image of an object and function with its name.
- At the second stage, the emphasis in rehabilitation is on the restoration of situationally determined speech. The patient is given a set of classes, including on-site orientation with verbal instructions from a specialist, and discussion of various everyday topics. To consolidate the results obtained, self-testing, questionnaires and classes with rehabilitation specialists are carried out.
- The last stage is aimed at improving visual and auditory-verbal memory. The patient is asked to solve crosswords and riddles, retell passages from books or conversations, and write stories. Conduct classes to improve factual memory by remembering important dates, addresses and other information. Communication with loved ones is important, since active speech and its perception help the patient restore the functions of various parts of the brain.
In addition to these activities, all patients need constant work activity, reading books and attending physical therapy classes. The rehabilitation process lasts from several months to several years, depending on the severity of the brain damage.