What do we mean by speech impairment? The question requires thought, because it is not so easy to decide what is considered speech and at what age speech should be formed in a child. Scientists studying communications have come to the conclusion that many animals can communicate with each other. Dolphins, dogs, and primates have their own language. But speech as a means of verbal communication is accessible only to humans. Of course, provided that he is used to communicating from a very early age. To prevent you from growing up Mowgli, help your child develop speech! Should we sound the alarm if a 2-year-old child cannot construct a coherent sentence or is this normal for his age? But your parents tell you that you are his age... And your friend’s son already tirelessly chats with his parents all day long. How to understand where are individual norms and where are deviations and disorders of speech development? We will talk about this below.
Stages of development and formation of speech in a child
The skills and inclinations of a normally developing child directly depend on his age. But even in infants, experts are able to predict speech disorders in the future based on some signs. If motor development in the first year of life lags behind the norm, this is a possible sign that speech and mental development will also lag behind. We would also like to note that development standards were established in Soviet times and were quite strict. Now, unfortunately, many modern children do not meet them. Children of the new generation speak less and their speech takes longer to develop. The reasons for this are global “gadgetization” and the transition of people to virtual methods of communication.
| Age | Skills |
| up to 6 months |
|
| 6-9 months |
|
| 9 months-1 year |
|
| 1-1.5 years |
|
| 1.5-2 years |
|
| 2-3 years |
|
| 3-5 years |
|
Experts recommend regular examinations to identify delays, if any, as early as possible. One child is one of those who “harnesses slowly and rushes quickly.” He will start speaking later, but within a month he will catch up and surpass his peers. Then consider yourself lucky. But for another child, prolonged silence may hide such gloomy diagnoses as autism spectrum disorder, alalia and others. And it is very important not to miss them and start correction on time.
If you have any doubts about whether your child’s development rate is within the normal range, it is better to visit a specialist. What if he has a general
speech disorder
(general speech underdevelopment - GSD) or delayed speech development (SDD)?
For a child with severe speech impairment
It is often difficult to perceive the world around us positively. He grows up as a gloomy beech, touchy and aggressive, feels insecure, and with age begins to feel his inferiority. You can read more about the symptoms and degrees of speech underdevelopment here. Consult with specialists! Both minor and more significant speech deviations are usually identified in the first few years of life as a result of comprehensive diagnostics.
The spheres and areas of responsibility of specialists in speech problems are distributed as follows:
- Speech therapist
: Consults from 1.5 years old, conducts classes from 2 years old. At the consultation, he makes a final diagnosis, if it is a disease, and refers to a neurologist if there are suspicions of disorders of a corresponding nature; - Speech pathologist
: works with non-speaking children; in case of delays in psycho-speech development and pre-speech diseases (alalia, autism spectrum disorder), it helps to “start” speech and develop other cognitive functions to the level of the age norm.
We are primarily talking about young children. also occur in adults
- due to a brain injury or stroke.
Their correction is carried out by speech therapists and aphasiologists. Sometimes speech impairment in schoolchildren
and adults remains from neglected/undertreated pronunciation defects in childhood.
Characteristics of speech tempo, types of speed disorders of speech function
Speech tempo is a characteristic property of speech that reflects the speed at which sounds are produced during a conversation. Speech tempo may be disrupted in the form of acceleration or deceleration, as well as stuttering. It depends on the speed of pronunciation of sound units that follow each other, as well as on the number and duration of pauses between words or sentences. The optimal speech rate for a healthy child or adult is 9-14 sound units per second. If a healthy patient increases the speed of speech, the frequency of pronouncing sound units increases to 15-20. At the same time, speech remains intelligible.
Types of changes:
- Tahilalia.
- Bradylalia.
- Stuttering.
Preschoolers have a tendency to accelerate speech, which can be explained by the immaturity of the inhibitory mechanisms of the brain and reduced control over speech. The reason for the increase in the rate of speech may be haste in speech among family members. In this case, the child gets used to speaking quickly. During puberty, the speed of sound reproduction may increase further. In patients with neuroses and other psychiatric diseases, rapid speech often provokes stuttering.
Increasing the speed of sound reproduction in a child inhibits the development of speech function. This leads to incorrect sound pronunciation and decreased intelligibility of words. If help is not provided in time, the patient will speak incorrectly and quickly throughout his life.
The concept of tachylalia, clinical manifestations of pathology, etiology
Tahilalia is an acceleration of speech with a frequency of 20-30 sound units. The disease develops due to changes in the functioning of the extrapyramidal system. According to scientist D. Weiss, accelerated speech provokes stuttering. Tachylalia can be inherited.
M.E. Khvattsev associates the occurrence of rapid speech with pathology of the articulatory apparatus, incorrect speech of relatives, untimely correction of the child’s speech function, and attention deficit. A. Liebmann considered the cause of tachylalia to be a lack of motor skills and auditory perception.
A patient with tachylalia speaks very quickly, making it difficult to concentrate. During a conversation, the child appears to hesitate, repeat what has already been said, swallow sounds, replace syllables, and unclear construction of phrases and sentences. But, if you draw the child’s attention to the incorrectness of speech, all errors disappear. Symptoms may intensify with excitement, while talking with strangers, during an argument, or during public speaking.
The patient experiences changes in writing and reading. Children with accelerated speech rearrange syllables and letters while writing, and replace words with similar sounds and spellings. The movements of patients with tachylalia are fast and abrupt. During sleep, the patient may rush around the bed. Many patients experience tics, hyperactivity syndrome, memory and attention deficits.
A child with tachylalia is excitable and quick-tempered. When excited, the patient experiences redness of the skin on the face, sweating, and coldness of the extremities. The patient is often uncontrollable and undisciplined. Such a child has a reduced ability to learn at school.
An increase in the rate of speech is accompanied by changes in the motor sphere, autonomics, and mental processes. The patient may also experience a lack of willpower and a disturbance in the emotional sphere.
The concept of bradyllalia, clinical manifestations
Bradylalia is a pathology of speech function in which the patient speaks at a slow pace (less than 9-14 sound units per second). There are long pauses between words and sentences, words are greatly stretched out during their reproduction. The disease can occur on its own or be a symptom of an underlying disease: nervous system pathology, head injury, brain tumor. When slow speech is a symptom of another disease, the patient experiences inhibition of motor function, asthenia, lethargy, and weakness. On its own, bradyllia occurs in slow and phlegmatic children and patients living in northern latitudes.
Speech signs of bradyllalia include slow speech, leisurely reading and writing. The child reads monotonously with large intervals between words and sentences, words are stretched out. A patient with bradyllalia sometimes produces sounds with a nasal tone. It is very difficult for others to perceive the patient’s conversation, as attention decreases, fatigue and tension arise due to too slow pronunciation.
Non-speech signs of a reduced speech rate are characterized by a decrease in motor function (fine motor skills, general movements, facial expressions). The patient's movements are slow, poorly coordinated, incomplete, awkward. The patient has practically no facial expressions. Patients have impaired speech perception, decreased attention, memory, and impaired thinking.
Patients have poor spatial orientation and find it difficult to complete any instructions or tasks the first time. Children with slow speech have difficulty switching from one subject to another.
Concept of stuttering, clinical symptoms
Stuttering in speech therapy is a speech pathology in which the rhythm, tempo, and fluency of speech are changed due to convulsive contractile activity of the muscular apparatus that carries out articulation. Pathology manifests itself in childhood and puberty. Most often, the disease begins to manifest itself at 2-5 years of age.
Stuttering is caused by muscle spasms. They can be tonic or clonic. Tonic spasms make it difficult to move from one sound to another. Clonic seizures provoke the repetition of words, syllables and sound units.
The causes of stuttering are:
- Immaturity of the nervous system.
- Injuries in utero, during the birth of a baby.
- Mental trauma.
- Bilingualism in the family.
- Increased development of speech function, which does not correspond to the patient’s age.
- The presence of a person who stutters in the child’s environment.
Stuttering has several periods of formation. The initial stage of the disease is characterized by a very rare disturbance in the fluency of conversation. In this case, stuttering occurs only with strong excitement, anxiety, and excitement. At an early stage, the child does not realize the presence of a defect in speech function.
At the second stage of the disease formation, the process becomes chronic. The patient is aware of the presence of stuttering, but is not afraid to talk. At the third stage of pathology development, the smoothness of conversation is noticeably disrupted. It is difficult for the patient to reproduce sounds, but there is a desire to talk, and the patient does not develop fear when talking.
The fourth stage of stuttering is considered the most difficult. The patient tries to talk less, as he feels very uncomfortable during speech. Fear of speech is present, which affects the child’s psychology. Patients' communication suffers. Such patients have difficulty studying and working.
Types of speech disorders in children and adults
In speech therapy, several basic typifications are accepted - based on similar manifestations and sources. This helps to understand in which direction to look for the source of the problem and ways to correct speech impairment. Clinical and pedagogical classification
- Rhythm and tempo disorders: Stuttering (a deviation known since time immemorial. According to historians, the ancient Greek orator Demosthenes once suffered from a stutter, but persistently practiced making speeches by stuffing his mouth with small pebbles. Having learned to speak clearly with stones in his mouth, he developed an excellent articulation and self-confidence, thereby getting rid of the disease. Speech therapists still practice this method of correcting speech disorders).
- Dyslalia (in oral speech the child incorrectly pronounces or distorts individual sounds).
- Dysarthria (organs of articulation (lips, tongue) have critical limitations in mobility).
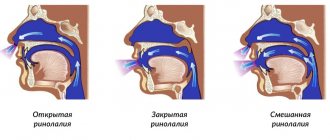
- Rhinolalia (reduced resonance in the nasal cavity).
- Other articulation disorders: polternium, tachylalia, bradyllalia.
- Aphonia (loss of a clear voice, a person speaks in a whisper. Problem with the vocal cords).
- Structural-semantic disorders: alalia (occurs during childbirth when the speech areas of the brain are damaged. At the same time, the child is fine with intelligence and hearing), aphasia (a similar problem. Organic lesions of the areas of the cerebral cortex that are responsible for controlling speech , and the adjacent “subcortex". It differs from alalia in that it is not a congenital phenomenon, but an acquired one - in people who can already speak. Usually occurs as a result of a stroke in adults).
- Dyslexia (difficulty perceiving written text, mixing sounds and words when reading, inability to form letters into ready-made words).
Psychological and pedagogical classification of speech disorders
- violations in the use of communication means stuttering
- other complications
- phonetic-phonemic speech underdevelopment
Forms of systemic speech underdevelopment
A mild degree of systemic speech underdevelopment is characterized by minor disturbances in sound pronunciation. The child begins to stammer only when he tries to say a complex phrase. He loses secondary lines of meaning in his attempts to convey the main idea. The child cannot use prepositions, “loses” conjunctions, does not always form the “noun-adjective” chain correctly, and gets confused in quantitative characteristics. Vocabulary is less than that of peers.
With an average degree of systemic underdevelopment of speech, the child “floats” in cases and genders and does not coordinate them with each other. As for speech, a violation is recorded only when trying to pronounce sounds of one group. Complex everyday words remain an unconquered peak for the baby. Words united by one semantic line are designated by the child as one word. For example, a sofa, a wardrobe, a TV, a carpet - this is all “home”.
Severe form of systemic speech underdevelopment.
The child cannot form a phrase from words, hence the incoherent speech. One sound can mean both “mother” and “eat”. The problem is in the pronunciation of several sound groups at once: voiced, voiceless, hissing, voiced - all are pronounced incorrectly. The child perceives speech with inhibition. The speech contains incorrect use of cases and numbers.
Systemic underdevelopment of speech against the background of mental retardation is complemented by increased physical activity, inability to concentrate, and poor memory.
Causes of speech impairment in children
The deviation can be congenital or acquired, physiological or purely psychological. The choice of correction method directly depends on this. Once upon a time, ideas about the sources of speech anomalies were quite chaotic. Professor Mikhail Khvattsev, one of the pioneers in speech therapy among our compatriots, made a major contribution to the systematization of the causes. He divided them into internal and external and introduced the following classification:
- organic (anatomical-physiological, morphological): organic central (brain lesions);
- organic peripheral (defects of hearing or articulation, cleft palate, dental defects);
- functional (psychogenic - problems with excitation and inhibition in the central nervous system);
Trouble does not come alone; problems on any front will inevitably grow into a whole bunch of accompanying complications. Khvattsev emphasized the close connection between organic and functional causes. If the sensory organs do not work properly, natural reflexes are poorly established. And vice versa, if there are already problems of a functional nature, then the development of organs will also slow down. Like the affected central nervous system, it does not contribute to the development of the periphery.
Depending on the stage at which the basis for speech dysfunctions arose, they are divided into:
- hereditary. Unfortunately, we do not always inherit a strong body from our parents. Children get many troubles “as a gift”, sometimes it is stuttering, various disorders of the speech zones in the cerebral cortex, problems with bite or the wrong number of teeth, defects in the palate, anomalies in the structure of the organs of articulation.
- congenital (intrauterine). Caused by complications during pregnancy. If a woman works in a hazardous industry, delays maternity leave until the last minute or unsuccessfully tries to terminate a pregnancy, if the embryo is forced to drink alcohol, tobacco and strong drugs with the mother, then all this will never benefit the baby. The first trimester is especially important, when the central nervous system is formed in the fetus.
- perinatal (birth) and postnatal (appear soon after birth). They arise due to complications during the very birth of the baby, due to premature birth, as a result of birth injuries, etc.
- others (manifest in the first years of a child’s life and later). Here the root of evil is either psychological, social and everyday factors, or serious illnesses (meningitis and other dangerous infections, diseases of the hearing organs, injuries to the brain and speech organs).
Please note: the risks to which a fetus is exposed at different stages of its development before birth, and an independent person after birth, are not the same. Obvious tips that mothers sometimes neglect:
- during pregnancy, take care of yourself more than usual, avoid injuries, shocks and the use of harmful substances;
- carefully choose a maternity hospital with modern equipment and skilled midwives;
- after birth, do not develop sores, even small ones, remember how vulnerable the fragile organism of a little man who has just come into this world is.
Article:
Currently, there has been significant progress in the development of speech therapy.
Based on psychological analysis, important data were obtained on the mechanisms of the most complex forms of speech pathology (aphasia, alalia, general speech underdevelopment, dysarthria). Alalia is one of the severe and persistent forms of speech pathology. Many children with alalia do not acquire language and remain non-speaking or barely speaking even after entering school. Thus, the problem of diagnosing and organizing correctional and educational work for alalia is one of the most important and fundamental scientific and pedagogical problems of the system of preschool and school educational institutions at the present time.
ALALIA is one of the most severe speech defects, in which the child is practically deprived of linguistic means of communication: his speech is not formed independently and without speech therapy assistance.
Alalia is the absence of speech or systemic underdevelopment of speech due to organic damage to the speech areas of the cerebral cortex in the prenatal or early period of a child’s development (before speech formation)
Alalik children represent a pedagogically heterogeneous group and differ in the severity of the defect and the productivity of correctional work.
Alalia is observed in children with intact peripheral hearing and articulation apparatus, who have sufficient intellectual capabilities for speech development.
Lack of speech sharply limits the child’s full development and communication with others. And this, in turn, leads to a gradual lag in mental development, which in this case is of a secondary nature.
With alalia, speech may be completely absent - the child is simply silent, or he utters individual inarticulate words that are incomprehensible to others.
Let's briefly look at how speech is formed normally:
— The first words appear about a year ago.
By the age of two, children should be able to communicate in short, simple sentences. These sentences, of course, are still very imperfect; there may be omissions of words that the child does not yet know. Many words are pronounced distorted and sound very funny. At this age, children master the sound composition of words and learn to formulate their statements grammatically correctly.
— At three years old, a child should speak quite competently, in full sentences, almost like an adult. The only difference is that his speech will express his still limited life experience. Incorrect pronunciation of individual sounds at this age is natural and is not considered a deviation from the norm.
The causes of speech formation disorders are associated with organic lesions of the central nervous system. These include:
- inflammatory, traumatic brain lesions
- birth injuries
- asphyxia
- intrauterine encephalitis, meningitis
- cerebral hemorrhages due to difficult and rapid labor
- unfavorable development conditions
- fetal intoxication
- congenital burden.
In addition, the occurrence of alalia is possible in children who have suffered severe rickets, complex diseases of the respiratory system, who had sleep and nutritional disorders in the early months of life.
Depending on the predominant localization of damage to the speech areas of the cerebral hemispheres (Broca's center and Wernicke's center), two forms of alalia are distinguished: motor and sensory, and recently the sensorimotor form of alalia has very often occurred.
Motor alalia
Motor alalia is a systemic underdevelopment of expressive speech (active oral utterance) of a central organic nature, caused by damage to the speech areas of the cerebral cortex in the prenatal or early period of speech development. This violation is due to the immaturity of linguistic operations in the process of generating speech utterances with the relative preservation of semantic and sensorimotor operations.
Motor alalia - the child understands speech addressed to him, but does not know how to reproduce it. (Parents say about such children: “He understands everything, but cannot say it.” ).
Sensory alalia
Sensory alalia is a systemic underdevelopment of speech that occurs with organic damage to the speech zones of the CGM (temporal region of the dominant hemisphere) and is caused by the immaturity of the operations of the process of perceiving addressed speech with the relative preservation of physical hearing and motor capabilities.
Sensory alalia - a child does not understand speech addressed to him (impaired perception and understanding of someone else's speech). Such children exhibit echolalia - automatic repetition of other people's words. Instead of answering the question, the child repeats the question itself.
Symptoms of motor alalia
Speech symptoms:
Children suffering from this form of alalia have sufficient pronunciation capabilities, but they are not able to use them. The disorders are phonemic in nature; the operation of selecting a sound to form a speech utterance is impaired. In the speech of motor alalitics, literal paraphasia (replacement of a sound in a word with another), perseveration (obsessive reproduction of sounds or words), and elision (loss of sounds) abound.
There are also violations of the semantic aspect of speech. These children have significantly more words in their passive vocabulary than they use in active speech. There is a predominance of subject vocabulary, while the verb vocabulary is sharply limited, both the understanding of verbs and the use in speech.
Children replace some words with others that are close in meaning and included in the same associative field with them, for example, instead of the word table they say chair, etc. Contamination can be observed in speech when a child in speech combines syllables belonging to different words into one for example, the word “trashet” means the tractor is plowing.
Violation of the grammatical structure of speech is manifested in incorrect agreement of words in number, gender, case, and tense. Children omit prepositions in their speech. Most motor speakers understand spoken speech at the nominative level (they mostly know the names of objects).
Non-speech symptoms:
Severe neurological disorders are observed:
- Oral apraxia (motor disturbances of purposeful movements and actions of the facial muscles with a disorder of complex movements of the lips and tongue).
- General motor clumsiness; children with motor alalia have impaired balance.
- Impaired fine motor skills.
- Signs of minimal brain dysfunction.
- pronounced vegetative-vascular changes.
Psychopathological symptoms:
- Speech negativism (reluctance to speak) is very characteristic.
- The mental development of children lags behind the norm to varying degrees.
- Higher mental functions (memory,
attention, thinking, etc.).
- Local lesions of the cerebral cortex also affect nearby
speech zones.
- It is difficult to program one’s actions; there is a decrease in
arbitrariness of actions.
- Children can be inhibited, but more often they are disinhibited and impulsive.
- They adapt poorly to the conditions that surround them.
- There is a pronounced lack of formation of game actions.
- Children are touchy, withdrawn and often aggressive.
A child cannot learn to speak due to poor control of his speech organs (tongue, lips, lower jaw).
At the same time, his muscles are absolutely healthy, he simply cannot act with them at his own discretion (voluntarily). Moreover, he fails, or only poorly succeeds in speech movements (he cannot pronounce speech sounds, and therefore words), but non-speech movements are in perfect order (he opens his mouth while eating, chews, licks, smiles, etc. .).
Speech understanding is intact in this form of alalia.
Symptoms of sensory alalia
Speech symptoms: the primary violation in the structure of the defect is a violation of phonemic perception of varying degrees: from complete insensitivity to speech sounds to difficulty distinguishing words that sound similar in sound. Passive vocabulary is practically absent. In everyday situations, the child is more likely to focus on intonation, sequence of actions, etc., but not on words. Impressive agrammatism blocks the formation of one's own speech. Logorrhea and echolalia are noted.
Non-speech symptoms. Neurological disorders: sensory-acoustic syndrome (flickering inconstancy of auditory function), auditory agnosia, hyperacusis, specific behavioral and movement disorders.
Psychopathological disorders: the cognitive sphere suffers to a greater extent than with motor alalia. Nonverbal processes develop only through visual processes and display. Severe developmental retardation is often noted. Behavior is chaotic, chaotic, impulsive. A child cannot learn to speak because he does not distinguish between the sounds of speech; it is as if he “does not hear” . At the same time, he hears any other “non-speech” sounds very well and reacts to them.
Such a child usually lacks his own speech completely, or there may be individual babbling words, or there may be echolalia (when he repeats a word he has just heard, if he is able to remember it for a short period).
Since the child does not perceive the sounds of speech, he does not understand the speech of others.
Motor alalia can be expressed to varying degrees depending on the severity of the neurological disorder, the conditions of upbringing and speech environment, the time and duration of speech therapy, and also largely depends on the compensatory capabilities of the child: mental activity, state of intelligence and emotional-volitional sphere.
- degree The child is not able to make any voluntary movements with the organs of speech, even just to open his mouth upon instructions. However, the same involuntary actions are not affected (that is, he opens and closes his mouth perfectly while eating). With such severity of the disorder, the child, as a rule, does not speak at all or makes inarticulate sounds.
- degree The child is able to make simple voluntary movements with the speech organs (copy them). In this case, he may develop some speech. He can very imperfectly pronounce a limited number of words consisting of individual syllables and sound combinations. The same word can be pronounced differently each time, since he does not remember the speech movements that comprise it.
To understand whether a child has motor alalia, you need to determine how well he controls his speech organs. Check if he can imitate (follow you in your demonstration) certain movements with the speech organs: open and close his mouth, stick his tongue out of his mouth and put it back, smile and stretch his lips into a tube, raise his tongue up to his teeth and lower it down. Movement is needed
perform while looking in the mirror. If the child cannot cope with these actions, check whether he is generally able to perform at least some movements with his speech organs according to the instructions. For example: ask him to open his mouth, show this action several times, tell him to imagine how he eats, bring a spoon to his mouth. Or: smile, pretend to laugh, invite your child to laugh together.
Sensory alalia can be expressed to varying degrees.
1st degree
The child may not perceive speech sounds completely - may not pay attention to them. Then he does not react at all to speech and gives the impression of being deaf and mute.
2nd degree
The child may have no reaction to the human voice at all. He does not hear or distinguish people's voices.
3rd degree
A child can perceive some speech sounds and their combinations, but it is very difficult to distinguish between them. Then he responds to verbal appeals, but still does not understand their meaning or understands it very distantly.
Basically, he orients himself based on the situation, reacting to the gestures of the people around him, facial expressions, turns of the head, and roughly guesses what is being said and what is happening. In this case, parents may consider that the child has a completely satisfactory understanding of speech.
To determine if a child has sensory alalia, you need to check if he understands simple instructions and the meaning of words. Invite him to perform well-known actions (approach something, bring something, etc.). Ask to show this or that thing (window, table), to make this or that movement (sit down, lie down, walk). All instructions must be in exclusively verbal form, completely avoid any kind of gestures: pointing gestures, turning the head, looking at the object. Also check how your child reacts to speech sounds and human voices. Call him behind his back (hey, ow), pronounce vowels and consonants and see if they attract his attention. A child who cannot understand speech must have his physical hearing tested.
Sensorimotor alalia
This speech disorder is a combination of the auditory and motor disorders described above, expressed to varying degrees, and is therefore the most severe speech defect.
In this condition, the child does not understand foreign speech, does not have the ability to recognize it, and cannot speak. Sensorimotor alalia occurs in approximately 3.7% of all cases of the disease.
Treatment of alalia in children
Treatment of alalia in children is carried out under the supervision of a pediatric neurologist and psychiatrist. Regular sessions with speech therapists play a huge role. Parents should treat such a child with care and understanding. However, there is a fine line beyond which lies the recognition of the child’s inferiority. Treat him like an ordinary baby, but at the same time take into account the peculiarities of his development.
Of decisive importance in the treatment and education of children with alalia is the plasticity of the child’s brain - the ability of healthy brain cells to replace those that, for one reason or another, are not included get to work. The nerve cells of the cerebral cortex, which are responsible for higher mental functions, do not have innate specialization. There is only an innate preparedness of nerve cells for some type of activity. But if necessary, you can force “healthy” structures intended for one thing to do something else. This is possible provided that the nerve pathways connecting individual parts of the brain are preserved. During the period of speech development, their condition is more important than the condition of the speech zones themselves. The plasticity of the child’s brain fundamentally distinguishes it from the adult, whose intact areas are difficult to include in the compensatory process. It is the plasticity of nervous tissues in childhood that allows us to help children with alalia. Even in the most severe cases of alalia, the situation is not hopeless if treatment is started on time. It is believed that differentiation and maturation of cerebral cortex cells takes up to 9 years. It is important to begin multiple complex treatments long before this. Banal knowledge of normal speech development (the timely appearance of humming, babbling, words, phrases) should contribute to the early referral of a child with delayed speech development to specialists: a neurologist, a psychiatrist, a speech therapist. Treatment of alalia is always complex, carried out by a group of specialists, including speech therapy, drug treatment, massage, physiotherapy, psychological and psychotherapeutic correction. Drug treatment should be intensive and amount to 3-4 courses per year.
Doctors have long known about the effectiveness of nootropics in the treatment of this pathology.
Speech therapy work is structured differently for motor and sensory alalia. But, in both cases, it should be started as early as possible, because without the help of a qualified specialist, the child’s speech will not be formed. Corrective work for alalia is long-term and requires systematic training and strict completion of homework, that is, close cooperation between parents and a speech therapist.
Parents of an alalik child should take speech therapy classes very seriously. Since alalia is a systemic underdevelopment of speech, speech therapy work should cover all aspects of speech.
Prevention of speech disorders. Helping a child at home
To prevent violations and for the general development of speech, constant communication is needed. Otherwise, problems will arise sooner or later, even if there were no medical prerequisites initially. A child learning a language must practice through regular contact with native speakers. And the carriers are you. Communication is an integral part of the education program.
What's useful:
- read together with your child, talk about what you read, illustrate the plot together, discuss the drawings;
- sing songs together;
- listen to the little why, without interrupting, answer his questions about the world around him, teach him to listen to others;
- correct errors in the pronunciation of words and sounds, find the correct analogues for “baby” words and “lisping” (“bobo”, “kaka”).
Mistakes that many people make, but I want to believe you don’t:
- the child’s questions are answered with the general “when you grow up, you’ll know” and “because it ends in U”;
- do little socializing and reading aloud; so that the child is not distracted from his work, they turn on cartoons for the whole day and leave him alone with the TV or computer;
- They repeat with tenderness after the baby everything that he babbles, thereby contributing to the reinforcement of incorrect words and illiterate pronunciation - they impoverish the speech of the future native speaker of the Russian language.
From a “technical” point of view, breathing exercises and tongue exercises are always beneficial. Breathing can be trained using play methods that are interesting to the child: blowing soap bubbles and balloons, learning to play toy flutes and harmonicas. There are standard articulation exercises for practicing various problem sounds, when the tongue, lips and teeth are held for 10-20 seconds in certain positions:
- sound “R” - mouth wide open, tongue at the upper jaw, tapping on the teeth while pronouncing the sound “D”;
- hissing - the lips are extended forward as much as possible, the jaws are closed;
- whistling - the end of the tongue rests against the front teeth of the lower jaw, and the edges against the far teeth of the upper jaw.
When we are talking not about prevention, but about the correction of already established deviations, the work is carried out more deeply, according to individual programs, with the regular participation of a speech therapist. If your child has clear signs of a speech disorder, but you cannot understand the reasons and what to do next, we suggest that you undergo a comprehensive diagnosis of speech disorders at our Center. To make an appointment for an examination and an appointment with a speech therapist, call tel. or use the online registration form on the website e.
Therapeutic measures
Treatment measures include eliminating the causes of speech dysfunction, as well as corrective work. If a child has a pathology that has caused a change in speech, he is first prescribed a course of treatment. Upon completion of therapy for the underlying disease, the patient is referred to a speech therapist. The speech therapist draws up a plan for speech therapy sessions. Correction is carried out both at home and in educational institutions. The number of classes is determined by the severity of speech disorders.
For bradyllalia, speech therapy classes are aimed at developing a faster pace of conversation and training the articulatory and motor apparatus. The speech therapist teaches the child to write, read, and clearly pronounce phrases and sentences faster. The classes train memory and attention. Outdoor games, skits, and dialogues are actively used, which help accelerate the pace of speech function. A good effect from the correction can be expected after 4 weeks. During a monthly course of therapy, speech speed becomes faster and pronunciation becomes clearer.
Children with slow speech need to conduct independent studies at home and control their conversation.
When treating tachylalia, a speech therapist conducts classes that include breathing training (slow, even), reading, and orderly, calm speech. The specialist teaches the child to work with a team, organizing performances in front of a group of people or children. During classes, they must develop general, auditory attention and train diction. The course of treatment for preschoolers and primary school students is 6-12 months.
It is better to correct tachylalia as early as possible (before 5 years of age), since therapy is less effective during puberty.
Stuttering correction is carried out at home and in the speech therapist's office. Family members need to avoid conflict and speak slowly and clearly. During treatment, it is better to refrain from visiting kindergarten for 2 months, events, and holidays, so as not to excite the patient. The correction course includes physical activity (running, swimming, cycling). During classes, you need to practice counting (count clothespins by attaching them to paper cut out in the shape of a circle), and use silent games. For correction, tongue twisters, gymnastics for the articulation apparatus, and breathing exercises are used.
WHOM TO CONTACT?
Correction of speech defects is carried out by two specialists - a defectologist and a speech therapist.
A speech therapist is a specialist who restores the speech of patients who do not have any deviations in physical and mental health, as well as disorders of the central nervous system.
A defectologist is a doctor who not only teaches how to speak and pronounce sounds correctly, but also deals with the correction of developmental disorders. The task of this specialist includes several tasks - eliminating defects of the speech apparatus, teaching a person to communicate, overcoming barriers and life difficulties.
BASIC PRINCIPLES OF OPERATION OF THE CENTER IN KURSK
The center practices an individual approach to each patient, personal selection of diagnostic and correction methods. The specialists treat everyone who comes to the clinic with care and very patience, and always provide feedback to the parents of young patients. Parents are also consulted and useful recommendations are selected. After each lesson, a positive result is noticeable.
The network employs real professionals in their field. They have knowledge, skills and experience, therefore, they can provide quality assistance in each specific case.
It is important to understand that effective elimination of speech disorders is very important for every person. After all, it is speech that allows you to find your place in society and achieve certain heights. Every person should have this opportunity. Don’t delay your visit, call, make an appointment for your child and give him a future.
SIGNS OF SPEECH DEFECTS
There are certain signs that indicate the possible development of speech defects.
Expressive speech disorder – poor vocabulary, underdeveloped speech, poor perception and memorization of new words, misunderstanding of tense forms of verbs, reticence, use of the same phrases in conversation. In this case, the pronunciation of words can be correct.
Receptive language disorder – lack of interest in conversations. At the same time, the baby has difficulty following directions, often does not understand well what is being said to him, and cannot write or read what is written.
Corrective work with a speech therapist
By the age of 6-7 years, a child should correctly pronounce sounds, operate with a rich vocabulary (consisting of different parts of speech), construct consistent sentences (gender, number, cases), conduct dialogues and monologues. If there are any persistent disorders at 4 years old, it is better to consult a speech therapist.
If your child has impaired pronunciation (motor alalia, dysarthria or dyslalia is observed), you need to teach him to control the organs of articulation. This is really a lot of work for a child, because the central nervous system, brain and peripheral nervous system are involved. Sound pronunciation is corrected in 4 stages:
- Preparatory – the ability to hear sound correctly.
- Sound production is the skills of correct pronunciation of a single sound through articulation exercises.
- Automation - honing pronunciation, introducing sound into syllables.
- Differentiation – consolidation of auditory and articulatory skills.
In the main groups of kindergartens classes are conducted with speech therapists. There are speech therapy kindergartens for children, where increased attention is paid to the development of the articulation apparatus. Speech therapy sessions are even more necessary if a serious pathology is detected. There is a special adapted preschool program for children with severe speech impairments.