Prevalence of the problem
The disease is a common occurrence, most common in the practice of speech therapists.
According to various estimates, the average number of children with such problems in preschool age is 25-30%, in elementary grades – 17-20%, and in older age – 1%. Classes with a speech therapist are also required for adults who have suffered strokes, TBI, or multiple sclerosis. Most often, there are combined disorders of sound pronunciation that prevent further mastery of written speech. At the same time, the vocabulary can be replenished according to age, all cases are used correctly, the structure of syllable formation is not disrupted, speech is developed at a high level.
How to help your baby
Many causes of organic dyslalia can be eliminated by a dentist. Some (lack of primary incisors) disappear on their own with age. But unfortunately, there are also fatal anomalies.
An undeniable advantage of the NeuroSpectrum Center for Pediatric Speech Neurology and Rehabilitation is the possibility of a comprehensive examination of the child not only by a speech therapist, but also by doctors. The specialists of our Center are well acquainted with the latest techniques for correcting pathologies leading to motor dyslalia. This allows you to promptly notice problems that can be corrected and refer the patient to a doctor of the right profile.
Classification of dyslalia
The two main groups in this disease are mechanical (organic) and functional dyslalia, the first is associated with defects in the anatomical structure of the speech organs, the second with social factors or neurodynamic disorders in the cerebral cortex (they are reversible).
Functional dyslalia
Functional dyslalia is divided into three types:
- motor - in the central sections of the speech motor analyzer;
- sensory – in the central sections of the speech-auditory analyzer;
- sensorimotor – with the simultaneous presence of both options.
With the motor type, a phonetic defect occurs (the articulatory signs of sounds are not reproduced), that is, the lips and tongue move inaccurately, so the sounds are only approximate, and articulation disorders occur. With the sensory type, a phonemic effect occurs (the acoustic characteristics of sounds are not distinguished) - it is difficult for a person to distinguish acoustically similar phonemes by ear (hard/soft, hissing/whistling, etc.), so he replaces and mixes sounds, which interferes with the mastery of written speech, and leads to dysgraphia in the future.
In accordance with the above options, 3 groups arise:
- acoustic-phonemic dyslalia;
- articulatory-phonemic;
- articulatory-phonetic.
The last two groups are combined under the name articulatory dyslalia, and the first two under the term phonemic dyslalia.
In any of these categories, different degrees of complexity of the disease are possible - complex dyslalia (incorrect pronunciation of more than 4 sounds) and simple.
In each of the listed categories, it is possible to distinguish types of dyslalia according to one more feature - which sounds and from which articulatory groups are affected. If all confused and unpronounceable sounds are in one group (for example, only hissing or only whistling), monomorphic dyslalia occurs, and if from different ones, polymorphic.
Phonetic dyslalia is divided into several narrow subtypes depending on phonetic defects in the pronunciation of sounds of different groups:
- rhotacism - incorrect pronunciation of consonants [р] and [р'];
- sigmatism – problems with hissing [zh], [sh], [sch], [h] and whistling [s], [s'], [z], [z']
- lambdacism - incorrect pronunciation of [l] and [l'];
- gammacism – difficulties in using [g] and [g'];
- hitism - deficiencies in consonants [x] and [x'];
- kappacism – speech problems with the sounds [k] and [k'];
- iotacism - incorrect pronunciation [th];
- defects in deafening and voicing - when a child or adult replaces paired voiceless ones with a voiced one and vice versa;
- defects of hardness and softening - paired hard sounds change to soft consonants and vice versa.
There are also such concepts as paragammatism, parasigmatism, when there is an additional phonemic defect (a sound is replaced by another). Disorders with dyslalia can be complex and combined, for example, lambdacism is combined with rhotacism, sigmatism with rhotacism, and they both also have softening defects.
The causes of the disease in this case lie in social and biological factors:
- children imitate the speech of adults (hurried, dialectal);
- adults talk to children using lisps and baby talk, which interferes with the development of normal speech;
- bilingualism in the family;
- pedagogical neglect, the child being left to himself;
- general physical weakness of the child;
- unformed speech patterns;
- delayed speech development.
Mechanical dyslalia
The cause of this form of the disease is organic defects of the speech apparatus itself - lips, tongue, teeth, jaws. Mechanical dyslalia occurs due to congenital causes or as a result of diseases and injuries.
The most common defects of the peripheral articulatory apparatus (tongue and lips) causing speech problems are:
- short frenulum of the tongue – problems with upper lingual sounds;
- short frenulum of the upper lip;
- massive tongue (macroglossia) – observed in children with general underdevelopment;
- small and narrow tongue (microglossia) - observed in children with general underdevelopment;
- thick lips – problems with labial and labiodental sounds.
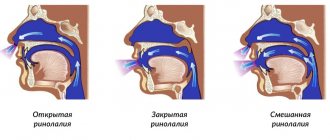
Causes of dyslalia in the inert part of the speech apparatus: high narrow or low flat upper palate, dental anomalies (sparse small teeth, diastema), malocclusion (open, deep, cross, etc.). Mechanical dyslalia is not diagnosed for cleft upper lip and soft/hard palate; speech defects in this case are classified as rhinolalia.
General information about mechanical dyslalia
Mechanical dyslalia occurs against the background of anatomical anomalies in the structure of the speech apparatus: lack of scars, malocclusion, serious pathologies of the dental system, underdevelopment of the tongue, lips or lower jaw, and others.
The phenomenon of dyslalia was first described at the beginning of the 19th century in Europe, but over time the description and definition changed. The most extensive description of speech features is found in the works of domestic specialists in the second half of the 20th century.
Mechanical dyslalia can occur at any age. Usually its presence does not prevent a person from living and communicating normally, but in some cases, pronunciation causes psychological discomfort and difficulties in communicating with people, so correction is necessary in any case. It involves a surgeon, an orthodontist and a speech therapist.
Symptoms of deviation
Dyslalia is characterized by a wide variety of symptoms represented by omissions (complete loss of speech), substitutions (substitution of a different sound each time it occurs), distortion (abnormal pronunciation) and confusion of sounds (pronunciation is sometimes correct, sometimes incorrect). Various symptoms appear depending on the form of the disease:
- with functional, the pronunciation of one or more sounds is impaired
- with mechanical - a group of sounds similar in articulation;
- with physiological, age-related tongue-tiedness is observed, the cause of which is the immaturity of phonemic hearing and the inability to correctly control the movements of the speech organs, which naturally goes away by the age of 5.
Diagnosis of dyslalia
Diagnosis of dyslalia by a speech therapist begins with finding out how pregnancy and childbirth proceeded, childhood diseases in the child himself, psychomotor and speech development at an early age, and excluding pathologies of hearing and vision. The organs of the articulatory apparatus are examined.
In the process of diagnostic work, identified pronunciation deficiencies are noted, the form and type of the disease is revealed. The ability to distinguish sounds is checked. If necessary, consultations with other specialists (dentist, orthodontist, neurologist, ENT specialist) are prescribed.
Causes
- defects and features of the development of speech organs;
- pedagogical neglect;
- violations of the mechanisms of perception, analysis and reproduction of speech (as a result of hearing loss, injury, etc.);
- the presence of a person around the child who cannot pronounce certain sounds well;
- abuse by parents of distorted “children’s” pseudo-words, such as “kisya”, “vava”, etc.
- use of two or more languages in the family.
The child usually pronounces most sounds and syllables correctly; the only difficulties for him are sounds that are similar in place and method of formation. The violation can manifest itself as one defect or a combination of them.
Complications
Complications of mechanical dyslalia include difficulties with socialization in childhood, which leads to inability to build relationships in the future.
Burr and nasality can cause ridicule from peers, and this is very painful for children. Psychological trauma underlies subsequent nervousness and complexes.
Mechanical dyslalia at school age causes difficulties with reading and writing, which, combined with psychological discomfort and self-doubt, lead to academic failure, refusal to learn, antisocial behavior and social maladjustment.
Prognosis and prevention
The prognosis for comprehensive, timely treatment of the disorder is positive in most cases. The sooner dyslalia of the mechanical type is eliminated, the greater the chance that the child will not lag behind his peers in academic performance and have problems with communication. The best age for correction is preschool.
Correction almost always takes a long time, during which all necessary medical and speech therapy procedures are carried out.
During this period, it is important not to discourage the child from studying, so the professionalism of the speech therapist and the support of parents are important here.
Prevention of mechanical dyslalia should begin at the stage of pregnancy planning, because many developmental anomalies are associated with the mother’s poor lifestyle, especially during the first trimester.
Preventive measures include timely contact with specialists.
For example, the first visit to the dentist should be planned for when the baby is 6 months old, so that you can anticipate possible problems with teeth or bite in the future.
If possible, artificial feeding should be avoided. If this is not possible, it is necessary to visit a pediatrician for prevention; from the moment the first words and phrases are uttered, take the child to a speech therapist.
Parents can do exercises and games aimed at expanding vocabulary, pronunciation and speech development at home on their own.
Mechanical dyslalia can be prevented from early childhood. This is a common pathology that becomes more and more noticeable over time for a child, teenager, or adult.
If the disease is left to take its course, in the future it can lead to conditions that are practically impossible to correct. To avoid serious complications, you need to pay attention to the child’s speech from early childhood and not ignore incorrect pronunciation, burrs and nasal sounds.
Related posts:
- Dyslalia - from diagnosis to effective treatment Dyslalia in childhood leads to negative consequences of speech development...
- Dyslalia - functional form Dyslalia is the most common speech disorder. This deviation...
- Rhoticism in speech - complete information Rhotacism (problem with the sound [P]) is the most common disorder in children...
- How to cope with dyslalia? There are different types of speech defects. Let's consider the features of dyslalia and its methods...