The emergence of speech in humans and the formation of sounds is possible thanks to the speech apparatus. The speech apparatus is a set of coordinated organs that help form the voice, regulate it and form it into meaningful expressions. Thus, the human speech apparatus includes all elements directly involved in the creation of sounds - the articulatory apparatus, including the central nervous system, respiratory organs - lungs and bronchi, throat and larynx, oral and nasal cavities.
The structure of the speech apparatus
The structure of the human speech apparatus, that is, its structure, is divided into two sections - the central and peripheral sections. The central link is the human brain with its synapses and nerves. The central speech apparatus also includes the higher parts of the central nervous system. The peripheral department, also known as the executive department, is a whole community of elements of the body that ensure the formation of voice and speech. Further, according to the structure, the peripheral part of the speech apparatus is divided into three subsections:
- The department that regulates respiratory processes. Breathing is an important function of the body. It is implemented by special nerve centers and occurs automatically. Sounds from the body always come out during exhalation, and the air wave formed at this moment helps to perform two tasks at once - articulatory function and voice formation. This section includes the lungs and bronchi, the muscles located between the ribs, and the diaphragm.
- Voice department. The voice has three characteristics. This is its power, timbre and height. The work of the vocal cords causes vibrations in the air, transmitted to the outside world, perceived as voice.
- The articulatory apparatus is the department that directly forms sounds into speech. Consists of active and passive organs. Active organs of articulation are movable, helping to form sounds. The main organs of articulation are the lips and tongue, palate and jaw. Their changes in position lead to the creation of narrowings in different places of the articulation department. The character of the sound produced depends on this position. The mandible helps create stressed vowels. The tongue is the main muscle of the articulatory apparatus. The clarity of pronounced sounds depends on its ability to be flexible and transformative. The lips are also a moving part and contribute to the formation of vowel sounds and speech, they are an important organ in the articulation of words, which is helped by the specific placement of the tongue.
Passive organs included in the articulatory apparatus are immobile organs. Their main task is to be the foundation, the basis for active organs. Passive organs include teeth and the entire oral cavity, and the hard palate. As well as the pharynx and larynx. Although they are motionless, they still influence, albeit slightly, the speech potential and character of a person’s speech.
Classification of vowel sounds.
The basis for the classification of vowels is the row and rise of the tongue, as well as the work of the lips. Articulatory vowels are distributed horizontally along the row, that is, along the part of the tongue that is raised when pronouncing a given sound. There are three rows, and accordingly three types of speech sounds, which are front, middle and back. Front vowels - and e; middle row - s; back row at o a. Vertically, vowels differ in their rise - that is, in the degree of elevation of one or another part of the tongue during the formation of a given vowel. There are usually three lifts - upper, middle and lower. In the Russian language, high vowels include u y, middle vowels e o, and low vowels a.
According to the position of the lips, vowels are divided into labial, that is, in the formation of which the lips take part - o u (labialized, rounded) and unglobbed, that is, in the formation of which the lips do not take part - a e and y. Labial vowels are usually back. Nasalization. In a number of languages, there are nasal vowels, for example, in French and Polish. Old Church Slavonic also featured nasal vowels, which in Cyrillic were represented by special letters: yus large, or o nasal and yus small, or e nasal. Articulation of nasal vowels occurs when raised? the palatine curtain and the lowered back of the tongue, so that the air stream simultaneously and equally enters the oral and nasal cavity.
Voice formation
In every language on our planet there is a specific number of sounds that create the acoustic image of the language. The sound finds meaning only in the scheme of sentences and helps to distinguish one letters from others. This sound is called a phoneme of the language. All sounds of a language differ in articulatory characteristics, that is, their difference comes from the formation of sounds in the human speech apparatus. And by acoustic characteristics - by differences in sound.
The voice can be considered the result of the hard work of the muscles of various components of the peripheral speech apparatus. Three of its departments contribute to the formation of sound:
- respiratory, otherwise energetic - includes the lungs, bronchi, trachea and throat;
- voice-forming department, otherwise generator - the larynx along with sound cords and muscles;
- sound-producing, otherwise resonator - the cavity of the oropharynx and nose.
The work of these departments of the speech apparatus in complete symbiosis can only occur through the central control of speech and voice-forming processes. This suggests that the respiratory process, articulatory mechanism and sound formation are completely controlled by the human nervous system. Its impact also extends to peripheral processes:
- the functioning of the respiratory organs regulates the power of the voice;
- the functioning of the oral cavity is responsible for the formation of vowels and consonants and for the difference in the articulatory process during their formation;
- The nose section provides adjustment of the overtones of the sound.
The central speech apparatus occupies a key place in the formation of the voice. The human jaw and lips, palate and supraglottic lobe, pharynx and lungs are all involved in the process. The air flow leaving the body, going further through the larynx and passing through the mouth and nose is the source of sound. On its way, the air passes through the vocal cords. If they are relaxed, then the sound is not formed and passes freely. If they are close and tense, the air creates vibration as it passes. The result of this process is sound. And then, with the work of the movable organs of the oral cavity, the direct formation of letters and words occurs.
Speech organs: normal structure and main pathologies - presentation
Author: Kotelnikova M.I.
The speech organs are divided into 2 groups: the respiratory organs (lungs with bronchi and trachea), which create the air stream necessary for sound production; organs directly involved in sound production, active (mobile), capable of changing the volume and shape of the vocal tract and creating obstacles in it for exhaled air, and passive (immobile), deprived of this ability.
1) The larynx, consisting of the cricoid, thyroid and two pyramidal or arytenoid cartilages and two pairs of muscle folds, of which the lower is called true vocal cords, the upper is false. The posterior end of each of the true vocal cords is connected to one of the arytenoid cartilages, the anterior ends converge at the inner corner of the thyroid cartilage. Thanks to the vibrations of these ligaments under the influence of exhaled air, a tone called voice appears. 2) The pharynx, which can narrow and expand. 3) Language used in the formation of various speech sounds. 4) Lips capable of various articulations. 5) The palatal curtain with a small tongue, which, rising, closes the passage to the nose and separates it. nasal cavity from the pharynx; when lowered, it leaves the passage into this cavity open
Teeth (upper and lower), hard palate, nasal cavity. All active organs can, by approaching or coming into contact with passive ones, as well as with each other, create a barrier to the exhaled stream of air. At the location of the obstacle, a source of noise is created, which is necessary for the formation of consonants. The teeth and hard palate are only the site of action of the active organs (tongue and upper lip). The nasal cavity serves as a resonator, which, when turned on, imparts a nasal character to the sound.
respiratory organs speech organs passive speech organs active brain
All speech sounds are formed only during exhalation. These are the lungs, bronchi, trachea, diaphragm, intercostal muscles. The lungs rest on the diaphragm, an elastic muscle that, when relaxed, has a dome shape. When the diaphragm and intercostal muscles contract, the volume of the chest increases and inhalation occurs when exhalation relaxes;
these are immobile organs that serve as a fulcrum for active organs. These are teeth, alveoli, hard palate, pharynx, nasal cavity, larynx;
These are mobile organs that perform the main work necessary for the formation of sound. These include the tongue, lips, soft palate, small uvula, epiglottis, vocal cords. The vocal cords are two small bundles of muscles attached to the cartilage of the larynx and located across it almost horizontally. They are elastic, can be relaxed and tense, and can be moved apart to different widths;
coordinates the work of the speech organs and subordinates the technique of pronunciation to the creative will of the speaker.
A child’s speech is formed under the influence of adult speech and depends on speech practice, speech environment, upbringing and training. Speech is not an innate ability, but develops in the process of individual development from the moment of birth to the end of life. Speech develops in parallel with the physical and mental development of the child and serves as an indicator of his overall development. The development of speech is closely related to the development of thinking.
To understand speech pathology, it is necessary to clearly understand the entire path of sequential speech development of children in normal conditions, to know the patterns of the process, to imagine each stage of speech development in order to notice deviations in this process.
Stage I of speech development - preparatory (from birth to one year) At this time, vocal reactions appear: screaming and crying, which contribute to the development of movements of the respiratory, vocal and articulatory apparatus. After two weeks, the child begins to respond to the speaker’s voice: he listens and stops crying.
By the end of the 1st month, the child can be calmed down with a melodic song. Next, he turns his head towards the speaker and follows him with his eyes. Soon the baby begins to react to intonation: to a gentle one he perks up, to a harsh one he cries. Around 2 months, humming appears, and by the beginning of the 3rd month, babbling (ahu, cha-cha, etc.) appears. From 5 months, the child hears sounds, sees articulation, and tries to imitate. From the age of 6 months, he pronounces individual syllables by imitation (ma-ma-ma, ba-ba-ba, etc.). Subsequently, the tone, rhythm, melody, and intonation of speech are adopted. In the 2nd half of the year, sound combinations are perceived and associated with objects and actions (tick-tock, bang, etc.), words are remembered, and reactions to them appear. From 7-9 months, the child repeats various sound combinations after adults. By the end of the 1st year of life, the first words appear.
Stage II – pre-preschool (from 1 year to 3 years). The stage of formation of active speech. At this time, the child willingly repeats after the speaker and pronounces the words himself. At the same time, it confuses sounds, rearranges them, distorts them, and skips them. From the age of 1.5 years, an understanding of an adult’s verbal explanation, the accumulation of new words, and the assimilation of knowledge appear.
By the age of 2, children master the skills of using singular and plural nouns, tense and person of verbs, and use case endings. In the second or third year of life, a significant accumulation of vocabulary occurs, the grammatical structure of speech is formed, and elements of coordination and subordination of words in a sentence appear. By the age of three, children should have formed all the basic grammatical categories. At this stage, speech understanding exceeds pronunciation capabilities.
Stage III - preschool (from 3 to 7 years) At this stage, children still have incorrect sound pronunciation. But sound control over one’s own pronunciation and the ability to correct it are already developing (i.e., phonemic perception is being formed). During this period, a rapid increase in vocabulary continues, the development of the grammatical structure of speech, mastery of coherent speech, and the structure of sentences becomes more complex. In the fifth year of life, children’s statements resemble a short story. At five years old, children, without additional questions, compose a retelling of a fairy tale from 40 to 50 sentences, which indicates mastery of monologue speech. During the same period, phonemic perception improves: vowels and consonants are distinguished; soft-hard consonants; sonorant, whistling, hissing sounds. By the age of five, the formation of correct pronunciation ends and the child speaks clearly.
Stage IV - school (from 7 to 17 years old) The main feature of the development of speech in children at this age is its conscious assimilation. Children master sound analysis and learn grammatical rules for constructing statements. In this case, the leading role belongs to written speech
These stages do not have strict, clear boundaries. Each of them smoothly transitions into the next. For the correct and timely development of speech, certain conditions are necessary. The child must be: * Mentally and somatically healthy * Have normal mental abilities * Have normal hearing and vision * Have a need for communication * Have a full-fledged speech environment
The full assimilation of writing and written speech is closely related to the level of development of oral speech. When speech is underdeveloped, writing and reading impairments of varying severity usually occur. The development of a child appears in several aspects related to the gradual acquisition of language: * Development of phonemic hearing and the formation of skills in pronouncing phonemes of the Russian language. * Mastery of vocabulary, grammar and syllabic structure of words * Mastery of the semantic side of speech.
* various intrauterine pathologies (toxicosis during pregnancy, viral and endocrine diseases, injuries, blood incompatibility according to the Rh factor, etc.). The most severe speech defects occur when fetal development is disrupted in the period from 4 weeks to 4 months. * Birth trauma and asphyxia (lack of oxygen to the brain due to respiratory failure) during childbirth, which leads to intracranial hemorrhage. * Various diseases in the first years of a child’s life. * Skull injuries accompanied by concussion. * Hereditary factors. In these cases, speech disorders may constitute only part of the general nervous system disorder and be combined with intellectual and motor impairment. * Unfavorable social and living conditions leading to pedagogical neglect, disturbances in the emotional-volitional sphere and deficits in speech development.
a psychophysiological approach to functional impairment, in which pathology should be understood as some resultant of a certain functional impairment and the demands on function from society.
Based on this understanding of pathology, speech pathology can be defined as a violation of speech activity caused by the immaturity or disruption of psychophysiological mechanisms that ensure the assimilation, production, reproduction and adequate perception of linguistic signs by a member of the linguistic community, and such a violation that is perceived by society (social group) and by itself by a person as a deviation from the social norm. Thus, what is very broadly and vaguely designated as speech pathology, when taking into account the psycholinguistic approach, can be designated as a disorder (pathology) of language ability.
In cases of speech pathology, we are faced with the question of the possibility or impossibility of communication (communication in general or adequate, effective communication). In other cases, we are talking only about whether it is correct, good, beautiful to speak, one way or another. Speech pathology should be contrasted with other deviations from the norms of speech use, such as slips of the tongue, rearrangements of word elements, confusion, and erroneous uses of words (paraphasia). This is important because facts observed in the study of speech pathology and facts of the same kind observed in the study of normal speech may turn out to be identical.
Progressive paralysis (one of the variants of syphilitic psychosis): difficulty articulating, slurred pronunciation. In the developed form - inability to understand figurative meanings, intonation unmodulation of speech.
Korsakoff psychosis: a severe memory disorder, reflected in speech, especially in the form of paraphasia (substitution of an inadequate word in place of a necessary one).
Pick's or Alzheimer's disease: noticeable stereotypical speech - statements consist of the same words and syntagmas, pronounced with the same intonation.
Epilepsy: slow and unclear speech, slurred speech and a tendency to perseveration (repetition), stereotyping, florid speech, an abundance of words in a diminutive form. In more severe forms, there is a poor vocabulary (oligophasia).
Schizophrenia: reasoning and thoroughness of speech. Replacing concrete concepts with abstract ones and vice versa. Semantic discontinuity or meaninglessness, usually while maintaining the grammatical integrity of the sentence. Phonetic monotony, or patients increase intonation on a secondary, auxiliary part of the statement to the detriment of the main semantic part. Repeating words spoken by the interlocutor (echolalia). Senseless shouting of the same word or statement (verbigeration). As you can see, the symptoms are very different, which reflects the variety of forms of schizophrenia
Manic-depressive psychosis: telegraphic style, sometimes turning into incoherence. Jumping ideas, speech being distracted by new subjects. The emergence of a large number of associations based on consonance, hence the abundance of rhyming words.
Speech disorders in mental retardation and developmental delays. They have been little studied psycholinguistically. We are primarily talking about oligophrenics (with varying degrees of severity of the defect - morons, imbeciles and idiots) and children with early organic disorders that cause the so-called alalia - absence or underdevelopment of speech. At the same time, this group includes children without obvious organic disorders or with peripheral disorders - the so-called general speech underdevelopment.
Speech disorders that are of a performing nature and associated with defects in the motor programming of speech or the implementation of a motor program (for example, stuttering). They are more often called phonation disorders. The following types of phonation disorders are distinguished:
Dysphonia is the absence or disorder of phonation due to pathological changes in the vocal apparatus. Bradylalia is a pathologically slow rate of speech. Some researchers use the term bradyphrasia.
Tahilalia is a pathologically accelerated rate of speech. This name comes from the Greek word tachus, which means quick, and lalia - speech.
Dyslalia is a violation of sound pronunciation with normal hearing and intact innervation of the speech apparatus.
Rhinolalia (from the Greek rhinos - nose, lalia - speech) is a violation of voice timbre and sound pronunciation caused by anatomical and physiological defects of the speech apparatus. The combination of sound articulation disorders with voice timbre disorders makes it possible to distinguish rhinolalia from dyslalia and rhinophonia (rhinophonia of speech sounds - a violation of the timbre of the voice with normal articulation of audible speech).
Violation of various types of speech, especially oral speech, as well as reading, writing, and internal speech, is observed in aphasia that occurs as a result of damage to the so-called speech zones of the cerebral cortex by a painful process. In patients with aphasia, the correct selection of words and their constituent speech sounds, the grammatical structure of independent speech and the understanding of speech addressed to the patient are impaired; at the same time, unlike dysarthria, the movement of the muscles of the tongue, vocal cords, etc., which ensure articulate pronunciation, is relatively weakly impaired. The speech of patients with aphasia is impoverished, the stock of words used is significantly limited. Some syllables and words are replaced by others, incorrect ones, and some syllables and words disappear from speech altogether. There are several main forms of aphasia: motor, sensory, etc.
Alalia is one of the most severe speech defects, in which the child is practically deprived of linguistic means of communication: his speech is not formed independently and without speech therapy assistance. Alalia (from Greek a - a particle meaning negation, and Lat. lаlia - speech) absence of speech or systemic underdevelopment of speech due to organic damage to the speech zones of the cerebral cortex in the prenatal or early period of a child’s development (before speech formation).
Language is a system of means of communication between people and ways of expressing thoughts. Speech is the process of a person’s practical use of language for the purpose of communicating with other people. Speech is a specifically human form of activity that uses the means of language. Speech arises and develops in a person in the process of his communication with people around him, thanks to which he masters the language of this environment. In their speech during mutual communication, people express thoughts and feelings using language. In the process of verbal communication over many generations, various national languages are created. The child acquires language in the process of communicating with adults and learns to use it in speech.
Special psychology: Bogdan N.N., Mogilnaya M.M.
Structural components of speech
Responsible for speech function:
- The sensory speech center is the perception of speech sounds, based on the sound discrimination system of the language; Wernicke's area in the left hemisphere of the brain is responsible for this process.
- The center of motor speech - Broca's area is responsible for it, thanks to it it is possible to reproduce sounds, words and phrases.
In this regard, in clinical psychology there is the concept of impressive speech, in other words, the understanding and presentation of oral and written speech. There is also the concept of expressive speech - that which is spoken out loud accompanied by a certain tempo, rhythm, and emotions.
In the process of speech formation, each person should have a clear understanding of the following subsystems of their native language:
- phonetics (what syllables, sound combinations can be, their correct structure and combination);
- syntax (understanding exactly how the relationships and combinations between words occur);
- vocabulary (knowledge of the vocabulary of the language)
- semantics (the ability to understand the meaning of words long before acquiring pronunciation skills);
- pragmatics (relationships between sign systems and those who use them).
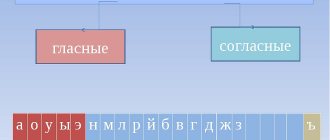
The phonological component of a language means knowledge of the semantic units of the language (phonemes). Physically, speech sounds can be divided into noises (consonants) and tones (vowels). Any language is based on a certain distinctive feature; if you change one of them, the meaning of the word will change dramatically. The main semantic distinguishing features include deafness and sonority, softness and hardness, as well as stress and unstress. It is these features that act as the basis of the phonemes of the language system. Each language has a different number of semantic units, usually from 11 to 141.
The Russian language involves the use of 42 phonemes, in particular, 6 vowels and 36 consonants.
It has been scientifically proven that any healthy infant in the first year of life has the ability to reproduce 75 different shortest sound units, in other words, can learn any language. But, most often, children at the initial stages of their development are in only one language environment, so over time they lose the ability to reproduce sounds that do not belong to their native Russian language.
Classification of consonant sounds.
The classification of consonants is more complex because there are more consonants in the world's languages than vowels. Noisy - sonorous. As part of the consonant sounds of any language, two large classes of consonants are distinguished: noisy, that is, sounds in the formation of which noise plays a major role, and sonorant, that is, sounds in the formation of which the main role is played by the voice arising from the vibration of the vocal cords. The difference between consonants according to the nature of the obstacle and the method of overcoming it. Consonants differ depending on what kind of barriers the speech organs form for the air flow coming from the lungs. If the speech organs are closed, then the air stream opens them. As a result, stop or plosive consonants appear. In those cases when the organs of speech are not closed, but only brought closer together, a gap remains between them. An air stream passes into this gap, characteristic air friction is formed, and the consonant sounds arising from this noise are called fricative (from the word gap), or fricative (from the Latin name fricare - “to rub”, since the air seems to rub against the gap in a loose manner). adjacent speech organs). In various languages there are also consonant sounds that combine the features of plosives with the features of fricative consonants. Such consonants seem to begin with a plosive element and end with a fricative element. They are called affricates. The Russian affricate ts consists of the plosive t and the fricative s, the affricate h - from the plosive t and the fricative sh. Africates are found in English (Georg), German (Deutsch) and many other languages. According to the method of formation of the barrier, trembling consonant sounds are also distinguished, during the formation of which the barrier is formed by periodically bringing the active organ of speech closer to the passive one until a very weak stop appears, which is immediately broken by a stream of air emerging from the lungs. If the first row of differences in the area of consonants is determined by the nature of the obstacles standing in the way of the air flow coming from the lungs, then the second row of differences is associated with the activity of the active organs of speech - the tongue and lips. According to this series of differences, consonants are divided into lingual and labial. When the front part of the tongue is involved in lingual articulations, anterior lingual consonants arise. Middle and back lingual consonants are also possible. The fragmentation continues: among the front-lingual consonants, dental consonants are distinguished, for example, t, and alveolar consonants, for example w). When articulating midlingual consonants, the middle part of the back of the tongue rises and moves closer to the hard palate (for example, the German so-called Ich-Laut in words like ich, Recht). When articulating posterior lingual sounds, the back of the tongue is brought closer together by the soft palate. The back-lingual ones include the Russians k, g, x. In addition to lingual, the same group of consonants also includes labial consonants, which in turn are divided into labiolabial (bilabial, for example, Russian p) or labiodental, for example, v). The difference between labiolabial and labiodental is easy to detect experimentally: to do this, you just need to pronounce the Russian sounds p and v several times in turn. The third row of differences in the system of consonant sounds is created by the so-called palatalization (from the Latin palatum - hard palate). Palatalization, or softness, is the result of raising the middle and anterior part of the tongue towards the hard palate. Any consonant, except for the middle ones, can be palatalized or softened. The presence of palatalized consonants is a striking feature of Russian phonetics.