Cerebral palsy is a disease that is characterized by typical disturbances in motor activity, as well as delayed development of the psyche and speech functions.
The cause of such disorders is damage to individual brain structures. The more pronounced the defect in the nervous system or areas of the brain, the stronger the functional impairment. Problems with speech formation are present in all variants of the disease. But the presence of full-fledged coherent speech directly affects the social adaptation, mental and intellectual development of the child. Therefore, one of the main tasks to compensate for the condition of cerebral palsy is to work on the development of high-quality speech function.
Causes of cerebral palsy
Cerebral palsy is formed in connection with various functional abnormalities in the brain, which can occur during gestation, during childbirth or the first months of a child’s life. A characteristic feature of the disease is its early manifestation, as well as the absence of further deterioration of the brain. However, of course, without proper care and timely corrective measures, the course of the disease will become more complicated.
The main causes of cerebral palsy are:
- Oxygen starvation (hypoxia) of the fetus.
- Infections suffered by the mother during pregnancy (for example, rubella, cytomegalovirus, toxoplasmosis).
- Complicated heredity.
- Rhesus conflict.
- Asphyxia or injury to the baby as a result of a difficult birth.
- Severe infections, head injury or toxic poisoning suffered at an early age.
Symptoms of cerebral palsy
The main and most typical symptoms of this disease include:
- Tension or, conversely, relaxation of muscles due to impaired tone.
- Uncontrolled paradoxical movements of the limbs - unexpected, sudden or slow.
- Skeletal deformities.
- Problems with vision or hearing.
- Impaired swallowing function due to improper muscle function.
- Delay (at different levels) of both speech development and intellectual and mental abilities.
- Cramps.
Not all children diagnosed with cerebral palsy have all of these symptoms. However, to a certain extent, many of them are present and require correction in order to help the child adapt in life.
Speech dysfunction in cerebral palsy
A large percentage of children diagnosed with cerebral palsy have disorders in speech formation. More often they do not act “alone”, at times they even combine with each other.
Main speech disorders in cerebral palsy:
- SRD—speech development delay.
- ZPRD - delayed psycho-speech development
- Dysarthria is incorrect sound pronunciation.
- Alalia is an absolute absence or delay in speech formation.
Speech disorders and developmental delays depend on the degree of brain damage, as well as delays in the formation of parts of the brain that coordinate speech activity. The child’s condition itself limits communication, gaining knowledge about the environment and skills in everyday activities, which, unfortunately, entails falling behind peers. The more important it becomes to take corrective measures that would help the child’s development from an early age and improve his ability to adapt to society.
An overly caring family upbringing also does a disservice, when parents anticipate the child’s wishes in everything, responding to his slightest gestures and instructions, without stimulating him to correctly form speech.
Features of the work of a defectologist
Speech therapy work for cerebral palsy is carried out using a specially developed methodology, taking into account the individual characteristics of the child’s psyche. A defectologist must use in his work the results of psychologist research indicating the degree of impairment of intellectual function. Classes are structured so that it is convenient for the child to perceive information.
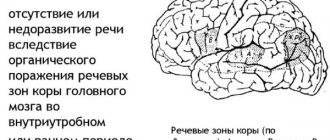
It should be remembered that speech disorders in sick children arise as a result of damage to certain areas of the brain responsible for speech functions. While the child is still small, correction of the consequences of this lesion occurs faster. As the patient gets older, the maturation of the “speech” areas of the brain is disrupted.
In parallel, disorders associated with pathological reflexes leading to articulation dysfunction and associated dyslexia should be corrected. After all, the more pronounced the defect in the functioning of the nervous system is, the stronger the functional impairment.
Treatment of cerebral palsy
In the treatment of cerebral palsy, complex therapy should be used. Medicines are used (to improve blood circulation in the brain, vascular, muscle relaxants, amino acids and vitamin complexes), therapeutic massage, physiotherapy, orthopedic and dynamic correction. However, in addition to restoring physiological functions, it is important to pay great attention to mental and speech development.
Here the main role is given to psychologists, neurologists and speech pathologists. The most important point in correction is to start as early as possible. The human brain develops very actively and is capable of delegating some of the work that the affected areas cannot do to other departments. This means that the child’s condition can be compensated for and adapted for life in society.
Article:
Studies by domestic and foreign clinicians note a delayed development of psychomotor functions in children with cerebral palsy, especially in the early stages of perinatal ontogenesis (K. Akosh, M. Akosh, L.O. Badalyan, D. Werner, I.I. Mamaichuk, E. M. Mastyukova, K.A. Semyonova, etc.).
L.M. Shipitsyn and I.I. Mamaichuk identifies 3 factors that influence the cognitive development of children with cerebral palsy:
— The relationship between sensory and cognitive development has a different basis for them.
“They are more limited in their research capabilities, as well as in receiving, storing and reproducing information adequate to their level of development.
— Painful experiences due to a long stay in the hospital, difficult relationships with parents, prejudiced attitudes towards others adversely affect the emotional and motivational sphere.
Since in cerebral palsy the leading defect is motor disorders that determine the specifics of the mental development of children, we will consider the features of the formation of the motor sphere in this pathology.
A feature of motor disorders in cerebral palsy is that they exist from birth and are closely related to sensory disorders, especially lack of sensation of one’s own movements. Motor disorders in children with cerebral palsy represent a unique deviation of motor development, which, without appropriate correction, has an adverse effect on the entire course of formation of the child’s neuropsychic functions.
In children with cerebral palsy, the formation of all motor functions is delayed or impaired: holding the head, sitting, standing, walking, and manipulative skills. Large variations in the timing of development of motor functions are associated with the form and severity of the disease, the state of intelligence, and the time of the beginning of systematic treatment and correction work.
To develop voluntary movements, skills and abilities, coordinated muscle work is needed. Muscles always work in certain patterns, the regulation of which is carried out by the central nervous system. An example of a normal movement would be sitting up from a supine position: bending the head to the chest occurs simultaneously with the flexion and rounding of the back, which allows you to sit up from a supine position. If you press your head against the pillow while lying on your back, your back straightens, becomes tense, and sitting down becomes impossible. A similar violation of the movement pattern occurs in children with cerebral palsy.
Thus, damage to the central nervous system affects the functioning of muscle patterns of voluntary movements, which determines one of the main difficulties in the formation of motor skills.
Incorrect movement patterns in children with cerebral palsy can become fixed and lead to the formation of pathological postures of the body and limbs. The most common incorrect postures are:
a) The head is raised up and thrown back, arms and legs are tense and straightened, the back is straightened. This position makes it difficult to sit up from a supine position, inhibits the development of upright standing, walking, and manipulative activities, which prevents the mastery of self-care, educational and work skills.
b) The head is turned to the right, the right arm and leg are extended, and the left ones are bent; or vice versa: the head is turned to the left. The left arm and leg are extended, and the right ones are bent.
These incorrect postures lead to the fact that the child cannot bend the arm towards which the face is turned, i.e. he is unable to examine the object taken in his hand. He does not develop the most important joint activity of the hand and eye for mental development—visual-motor coordination. This hinders the development of both voluntary movements, self-care skills, writing, and cognitive activity.
c) The head is lowered to the chest, arms and legs are bent. This position complicates the development of upright standing, walking, manipulative activities, and prevents the development of voluntary movements of the child.
All of these incorrect postures hinder the development of movements and self-care skills in children with cerebral palsy. They can also interfere with the child’s mastery of subject-related practical activities.
Sometimes incorrect postures and movement patterns are not clearly expressed, and their influence on voluntary movements begins to appear only in the process of developing more complex motor functions. However, in all cases, a characteristic feature of movement disorders in cerebral palsy is the dependence of movement disorders in the limbs on the position of the child’s head.
Some children with mildly impaired muscle tone experience apraxia (inability to perform purposeful practical actions). Such children have particular difficulty mastering self-care skills: dressing, undressing, fastening buttons, tying shoes, etc. Many people find it difficult to draw, design, etc. It should be noted that purposeful practical actions are formed in the process of motor experience.
The main manifestations of cerebral palsy are slowness and immaturity of motor skills and abilities. In some children, motor impairments are complicated by violent movements (hyperkinesis) of the head, arms, shoulders, facial grimaces, etc., which are especially intensified by excitement, fear, unexpected approach to the child, as well as when trying to perform certain purposeful actions.
The pathogenesis of cognitive impairment in children with cerebral palsy is extremely complex. Together with the pathology of the motor-kinesthetic functional system, sensory, intellectual and speech disorders observed in these patients play a significant role in the underdevelopment of perception.
Sensory perception includes the development of visual, auditory, tactile and kinesthetic perception (movement perception). Sensory perception is of great importance for the development of a child’s cognitive activity, for the formation of his higher mental functions, which is a necessary prerequisite for studying at school.
Children with cerebral palsy experience significant difficulties in spatial analysis and synthesis, disturbances in the body diagram, and difficulties in verbally reflecting spatial relationships. Without organized special training, children with cerebral palsy cannot learn individual features of the shape and size of objects. Comparative studies of the characteristics of tactile and visual perception in preschool children with cerebral palsy have shown that the basis for disturbances in the perception and representation of figures in children with cerebral palsy is a deficit in the integrative function of the brain. The severity of the motor defect is not always the determining factor in the underdevelopment of sensory-perceptual activity in these children.
Many children with cerebral palsy may have impaired touch sensation. The sensations from touching an object with the fingertips in such children are unclear; they are comparable to the impressions that a person experiences when he picks up an object while wearing thick gloves. Therefore, special games-exercises are needed to train tactile sensations.
A feature of motor disorders in cerebral palsy is not only the difficulty or impossibility of performing certain movements, but also the weakness of the sensations of these movements, and therefore the child does not form correct ideas about movement.
A weak sense of one’s movements and difficulty in handling objects are the cause of a lack of active sense of touch, including recognition of objects by touch (stereognosis). This prevents the formation of objective actions, which negatively affects the overall level of mental development of children with cerebral palsy.
In cerebral palsy, due to underdevelopment or decreased motor functions, there is a disruption in the activity of the auditory analyzer. Thus, there may be a decrease in hearing, which is most often observed in the presence of hyperkinesis. Particularly characteristic is a decrease in hearing for high-frequency tones and preservation for low-frequency ones. In this case, characteristic disturbances in sound pronunciation are observed.
A child who does not hear high-frequency sounds (t, k, s, p, e, f, w) has difficulty pronouncing them and skips them in speech or replaces them with other sounds. In the future, such children experience difficulties in learning to read and write.
Some children are characterized by insufficient phonemic hearing: they do not distinguish sounds and sound combinations that sound similar. For example, they can perceive words such as “goat” - “braid”, “house” - “tom”, etc. in the same way. In some cases, when there is no decrease in hearing acuity, there may be insufficiency of auditory perception and auditory memory.
Any impairment of auditory perception leads to speech delay, and in severe cases to speech underdevelopment.
It is very important to identify hearing impairment in cerebral palsy. Parents can be of great help with this. Early diagnosis of even slight hearing loss in a child with cerebral palsy is important to prevent mental retardation.
Some children have increased sensitivity to sound signals; they flinch at any unexpected sound, but their differentiated perception of sounds is insufficient. Using special pedagogical techniques, the child gradually overcomes fear when perceiving unexpected sound stimuli.
It is necessary to pay attention to the development of the baby's sensations, the subtlety and accuracy of which are inextricably linked with the development of his movements.
Visual perception in a child with cerebral palsy may be impaired due to limited eye movement, impaired gaze fixation, decreased field of vision, decreased visual acuity, etc., so it is difficult to look for an object, examine it and track its movement.
Prolonged, forced positioning in bed and impaired eye movements limit the field of vision in such children. Insufficient development of objective perception largely depends on the lack of objective actions in sick children.
It is known that actions with objects are formed as general motor skills improve. Thus, the child begins to actively manipulate objects when he holds his head well and sits steadily.
According to Shipitsyna L.M. and Mamaichuk I.I. severe visual impairment (low vision and blindness) occurs in approximately 10% of children with cerebral palsy.
In children with cerebral palsy (in approximately 20-30% of cases), strabismus, double vision, impaired coordination of eye movements, drooping upper eyelid (ptosis), and involuntary movements of the eyeballs (nystagmus) are noted. Such features of the visual analyzer lead to a defective, and in some cases to a distorted perception of objects and phenomena of the surrounding reality.
Some children, due to the presence of internal strabismus, get used to using a limited field of vision, ignoring its external fields. For example, with severe damage to the motor system of the left eye, a child may develop the habit of ignoring the left field of vision. When constructing from cubes or sticks, he does not complete the parts of the figure on the left, draws and writes only on the right side of the sheet, and when looking at pictures he also sees only the image on the right. The same violations are noted when reading. With such children in preschool age, it is necessary to conduct special classes on eye movements and holistic perception of an object.
For the formation of objective-practical and cognitive activity, the coordination of hand and eye movements is important. At the beginning, a healthy child, moving his hand within the field of vision, does not pay attention to it. Next, the gaze begins to follow the hand, and then direct the movements of the hand.
In children with cerebral palsy, as a result of damage to the motor sphere, as well as the muscular system of the eyes, coordinated movements of the hand and eye are insufficiently developed, especially if the above-described incorrect alignment of the body, head and limbs occurs. In this case, children are unable to follow their movements with their eyes, which hinders the development of manipulative activities, design and drawing, and subsequently inhibits the formation of educational skills (reading, writing) and cognitive activity.
The inability to follow the actions of one’s hands with one’s eyes and to coordinate the movements of the hand and eye leads to insufficient organization of a voluntary motor act. For this reason, the process of developing self-service skills slows down.
Movement disorders have a negative impact on the development of cognitive processes in children. For example, it has been shown that underdevelopment of spatial perceptions is observed in children with all forms of motor impairment (congenital and early acquired orthopedic diseases, myopathies and muscular dystrophies, flaccid paralysis). These disorders are temporary and can be easily compensated for when the child gains independent walking.
For many children with cerebral palsy, already from the first year of life, a disturbance in the process of active perception of the world around them is characteristic. A child with cerebral palsy cannot voluntarily turn his head, shift his gaze to this or that object, or grasp it.
Objective actions are an important form of a child’s active cognition of the world around him and the basis for the formation of sensory and mental processes.
Subject-based practical activities are actively developing in a child of the first year of life. R. A. Abramovich-Lekhtman identified four main stages in the formation of objective-practical actions in children of the first year of life. The first - the pre-action stage begins in the baby as early as 2.5 months. The child performs directed movements with objects: moves his hands along the blanket, grabs the other hand with one hand, etc. The stage of effective actions begins in the child at 4 months. The child masters grasping movements, after which a variety of objective actions become available to him: pulling, tapping, pushing, letting go, tearing paper and many others. After 7 months, the child can act with two objects at the same time: sticking in, putting in, taking out, stringing rings, etc. This is the stage of correlating actions. By the end of the first year of life, the child performs functional actions, imitating similar actions of adults: stirring a cup with a spoon, writing with a stick, combing a doll’s hair, etc.
Under the leadership of L.M. Shipitsyna and I.I. Mamaychuk conducted a longitudinal examination of children aged 0 to 3 years, who, according to the conclusion of neurologists, were at risk of developing cerebral palsy. In these children, specialists diagnosed cerebrovascular accidents of varying severity. They had a history of asphyxia, birth trauma, or asphyxia with birth trauma at the same time. Apgar scores in children ranged from 4 to 8 points.
Psychological examination was carried out at the age of 0 to 3 months, from 3 months. up to 6 months, and from 6 to 9 months. according to a specially developed scheme: study of sensations; substantive actions; voluntary activity.
The examined infants were divided into three groups based on their success in completing the tasks.
Group 1 (26.6%) included infants who did not experience significant disturbances in the development of sensations despite underdevelopment of motor functions; there was increased muscle tone and other neurological symptoms indicating cerebral-organic insufficiency of the type of cerebral palsy. There were no correlations between success in completing tasks and the severity of clinical manifestations.
Group 2 (48.8%) consisted of infants with delays in the formation of sensory functions. They experienced a complex of revival when an object was presented, but unlike the previous group, it manifested itself not in a reaction of concentration, but in erratic, chaotic movements of the limbs.
In group 3 (24.6%) there was a pronounced delay in the formation of visual and auditory concentration. The eye movements of these children were not coordinated with the turn of the head, and the hand movements were chaotic.
In the process of repeated examination of infants aged 3 to 6 months, an analysis of the interaction of vision and movement was carried out. By the end of the third month, a healthy baby begins to form connections between vision and hand movements. For example, simply looking at a baby's hand leads to an increase in its activity. The baby's hand, which accidentally enters the field of vision, lingers in front of the baby's eyes, and he tries to grab an object when the hand and the object simultaneously appear in his field of vision. At the age of 4 to 8 months of life, the activity of hand-eye interaction increases in children. Coordination of vision and grasping is a decisive step in the objectification of the object world in an infant and a trigger mechanism in the development of object-practical manipulations.
During this period, a healthy child actively develops grasping movements, which is an important prerequisite for the development of objective-practical actions. Actions such as grabbing, pulling, pushing, swinging, throwing, etc. are formed. The development of these actions is based on the formation of the intersensory hand-eye connection, which appears in a healthy child at 4 months and is an important trigger in the formation of subject-related practical actions.
Research so far has shown timely development of this type of connections (at 4 months) only in some children of the first group; in the remaining children, a lag in the development of intersensory hand-eye connections has been revealed by one and a half to two months. In all children of the second group, the intersensory connection of the hand also formed later than in healthy children, although many children could simultaneously hold an object and look at it. They experienced short-term concentration on the object, but quickly let it go. This is apparently connected, on the one hand, with the immaturity of the motor functions of the hands, and on the other, with a violation of attention. In the third group of children, the intersensory “hand-eye” connection was formed much later, in contrast to infants of the previous groups (in the period from 7 to 24 months). A sharp decrease in cognitive activity was observed in some children in this group, despite a fairly preserved range of hand movements.
An examination of the same children aged 6 to 9 months showed that correlating actions caused some difficulties in children of the first group, since their implementation required subtle and differentiated movements of the hand. However, in all children, cognitive activity was observed, they focused on objects for a longer time, actively picked them up, examined them, tried to transfer the object to the other hand, etc. In children of the second group, correlating actions appeared only by the end of the 1st year of life, but just like in the first group, they showed an interest in the object and a desire to pick it up. However, such actions as tapping, inserting, removing, etc. were practically inaccessible to them. In children of the third group, correlating actions began to form only in the 2nd year of the child’s life.
In the process of object-practical manipulations of the child, the researchers took into account not only the specifics and level of their development, but also the duration of concentration on objects and the emotional attitude towards them.
An important indicator of a baby’s voluntary activity is the characteristics of his attention. The first manifestations of a baby’s concentration appear on the 10th – 12th day after birth. By the end of the first month, the baby can already follow bright, shiny objects at a distance of 1 m from him. At 3 months, he listens longer to the sounds of a bell in his field of vision. At the 3rd month of life, the baby responds to the appearance of a person with a reaction of revival; from the 5th month, a certain object increasingly becomes the object of the child’s attention: a bright toy, a shiny ball, etc., which he manipulates.
The role of acting with objects to keep them in sight especially increases in a healthy child after 7 months. By the end of the 1st year of life, with the advent of walking, the child, performing functional actions with objects, can concentrate on them for 8-10 minutes.
The examination of infants at risk of developing cerebral palsy at the age of 6–9 months was aimed at analyzing their voluntary activity and attention. In children with cerebral palsy, in contrast to healthy peers, short-term concentration on objects was observed, especially in children of the third group (no more than 3 minutes). Of particular importance in the formation of stability of attention is the child’s search activity and the level of development of his substantive and practical actions. In the examined children, especially in the second group, cases were observed when the level of development of objective-practical manipulations was slightly reduced, search activity was observed, however, their attention was unstable and poorly concentrated. The greatest difficulties in concentrating attention were observed in the third group of infants. Unlike infants of the first and second groups, their underdevelopment of attention was closely correlated with the underdevelopment of object-practical manipulations. These data emphasize the totality of underdevelopment of all mental functions in infants of the third group.
A comparative analysis of the development of mental functions in healthy infants and infants with cerebral-organic insufficiency of the type of cerebral palsy showed the following:
- in healthy children in the first year of life, the development of mental functions is characterized by the most pronounced intensity, not only in the rate of their development, but also in qualitative transformations, especially in the second half of life. An important role in the formation of mental functions is played by the development of objective-practical manipulations, the level of development of which is closely related to the characteristics of voluntary activity;
— in children with cerebral-organic insufficiency of the type of cerebral palsy, there is, on the one hand, pronounced heterochrony in the development of mental functions, and on the other hand, their autonomy. Moreover, the more pronounced the autonomy of mental functions is, the lower the dynamics of the child’s mental development.
Thus, the leading defect in cerebral palsy - motor disorders - largely determines the specificity of the cognitive functions of children with this disease. The lack of development of motor skills and abilities is manifested not only due to impaired motor skills themselves, but also in the insufficiency of more complex functions necessary for cognitive activity, which are based on movement (visual-motor coordination, spatial analysis and synthesis, etc.)
Speech disorders occupy a special place in the structure of the defect in cerebral palsy. Speech development disorders in children with this pathology can be identified starting from the first months of the child’s life. First of all, this concerns the characteristics of the articulatory apparatus.
With cerebral palsy, already in the first days of life, the child experiences tension and trembling of the tongue. The tongue is almost not involved in the process of sucking and swallowing.
Typically, sucking reflexes are very weak or absent altogether. In these children, the appearance of these functions is complicated by the weakened state of the oral muscles and tube feeding. Subsequently, the oral reflexes that appeared with a delay are not reduced for a long time and are stored in a distorted form in the motor patterns of eating and articulation.
In this period of psychomotor development (0 - 1 month), postural reflexes directly influence the process of articulation formation. If a healthy child holds his head well, then in a child with cerebral palsy the reflexes of oral automatism may be excessively enhanced, general motor reactions (mainly holding and rotating the head) are inhibited, reflex-voice reactions do not acquire communicative significance, pseudobulbar symptoms are pronounced, characterized by disturbances in sucking, swallowing, breathing and screaming, and especially a violation of the Babkin hand-oral reflex. Children with cerebral palsy do not realize the possibilities of articulatory and facial motor skills.
At the 2-3rd month, a “revival complex” may be present in fragments. A smile is rarely observed when communicating with an adult. The pathology of the oral-articulatory muscles is significantly pronounced.
During the process of articulation, disturbances in muscle tone are clearly expressed in the form of paresis, spasticity, dystonia, hyperkinesis and tongue trembling.
In a cry, this symptomatology is clearly defined; it is very quiet, short-lived, and monotonous. Facial expressions are also less expressive and asymmetrical. In this regard, vocal activity is weak, very poor, humming appears late and the mechanisms of autoecholalia are not formed, humming is also delayed from several months to several years, depending on the level of disturbances.
During this period of psychomotor development (2–3 months), the motor component appears and general reflex reactions dominate. The rectifying labyrinthine reflex is clearly visible, which allows the child to raise his head when lying on his stomach. There is increased sensitivity in the oral cavity, especially the lips and tongue. Children with cerebral palsy have very pronounced pathological symptoms, primarily impaired sucking and swallowing.
At the age of 3 to 6 months, the “revival complex” is undifferentiated or absent, the cry is little expressive. The child reacts poorly to sound stimuli. There is no singing or laughter.
Booming is at a very rudimentary level, appears with a huge delay and is characterized by undifferentiated vowel sounds “a”, “e”, “s” that arise spontaneously when communicating with adults.
Children with cerebral palsy produce sounds that have absolutely no melodiousness, modulation or rhythm, which means that humming at this stage is weakly expressed (which is also facilitated by the absence of guttural sounds). More pronounced humming indicates a less severe form of cerebral palsy.
With pseudobulbar symptoms, disturbances in vocal production and cry persist. With spasticity of the articulatory muscles, increased tone of the tongue and lips appears. The tongue is tense, the tip of the tongue is not expressed, the lips are tense, which causes limitation of voluntary movements during articulation.
With hypotension, sluggishness of the masticatory and facial muscles of the articulatory muscles is noted. In children, it is not very mobile, as a result of which the mouth is constantly half open. In the case of dystonia, the muscles of articulation constantly contract, which is accompanied by hyperkinetic components.
In children with cerebral palsy, muscle hypertension is reflected in the pathological symptoms of the asymmetric cervical-tonic reflex. Pathological growth of tone in the muscles of the tongue and lips, sharp hypertension or hypotension, lack of voluntary movements of the organs of articulation, friendly movements, voluntary manual motor skills are clear indicators of a delay in the formation of motor activity, as well as in the appearance of chain rectifying reflexes.
In the period from 6 to 9 months of life, a child with cerebral palsy has difficulty distinguishing his mother from other people, often has negative emotional reactions to a new person, is inactive in communication, and has difficulty coming into contact with an adult in play. Does not use gestures during communication, facial expressions are unexpressive. Babbling has specific characteristics and can last for several years.
In this period (6–9 months), the presence of sensory and integrative connections is especially important. The chain motor reflex becomes the leading one in the development of a series of movements and the organization of a motor act. It is not only responsible for activating visual-motor manipulative behavior, but also affects the child’s spontaneous vocal reactions.
Children with cerebral palsy exhibit pronounced unconditioned reflexes of oral automatism. Biting and chewing are poorly expressed; particular difficulties arise with chewing, which is often completely absent.
The reactions of the tongue and lips are extremely inhibited. Often there are changes in the muscle tone of the lips and tongue and hyperkinesis of the tongue, which prevents mobility and the appearance of voluntary articulatory movements.
During meals, pseudobulbar symptoms are observed in the form of protective reflex reactions, oral synkinesis and increased salivation.
In the 5th period, from 9 to 12 months, a child with cerebral palsy exhibits weakly expressed emotional reactions. He prefers to communicate using gestures. In severe cases, the child shows little interest in the world around him. Low-active babbling (no more than 1-2 babbling words).
If in a healthy child babbling is finely differentiated according to the place and method of formation, then in children at risk of cerebral palsy the transition to expressive speech occurs much later, closer to two years. The babbling is little expressive, poorly differentiated, and poor in intonation shades. 2-3 syllables are extremely rare.
This period of psychomotor development (9 months) is characterized by differentiated sensory functions, which is reflected in rectifying reactions and control of movements. Oral movements become more differentiated, controlled and coordinated, although food still flows from the mouth during eating.
In children with cerebral palsy from 18 to 36 months. there is a violation of understanding both at the level of speech and at the level of gestures; there is no understanding of the meaning of the word “yes”, speech is poor, fragmentary, fragmentary, with articulation defects and the presence of perseverative echolalia.
Speech development disorders are expressed in “the poverty of their active and passive vocabulary, in undifferentiated knowledge of words,” children often confuse words denoting objects.
Speech, as the main means of communication, develops through movement and social contacts, and its foundation is laid in the first year of a child’s life. When a child suffers from a sensorimotor disorder due to cerebral palsy, the processes of articulation, sound pronunciation, control of facial expressions and gestures, kinesthetic perception, control of breathing and movement first of all change, and the ability of children to independently realize themselves in the world around them disappears. All this has a direct impact on the limitation of speech activity and mental development in general.
Children suffering from cerebral palsy have a violation of the phonemic system of speech, which leads to the inability to distinguish words that sound similar in sound. With low hearing acuity, there is often a lack of auditory memory and auditory perception. These disorders are directly related to delays and disturbances in the formation of articulation in cerebral palsy. A child who experiences difficulties in perceiving speech sounds and at the same time is limited in the ability to move speech muscles, also experiences difficulties in the process of articulation, which is especially characteristic of this pathology.
By the age of 2, with normal development, reflexes are reduced; characteristic of a child of the 1st year of life. Children with cerebral palsy at this time are still under the influence of reflexes. In severe forms, the asymmetric cervical-tonic reflex dominates, which is the most primitive and early. This reflex prevents the appearance and development of the cervical rectifier reflex.
Thus, the analysis of literary sources allows us to conclude that motor, cognitive and speech development in children with cerebral palsy is not just delayed in pace, but qualitatively impaired at every stage. Therefore, the most important factor in the successful development of a child is the earliest start of a well-structured, individually determined system of correctional work.