Production of sounds T - D when replaced with back-lingual K - Gplan summary on the topic
Production of sounds T - D when replaced with back-lingual K G
Our speech consists of sounds. A child must learn to correctly pronounce the sounds of his native language before school. In preschool age, the child’s pronunciation of sounds is observed incorrectly. This is a completely natural phenomenon. Three- to four-year-old children are characterized by a general immaturity of language. If you are not attentive to the child’s sound pronunciation, then such substitutions and distortions of sounds can remain for a long time.
For successful learning, a child needs intelligible and clear sound pronunciation. However, a large number of first-graders come to school with impaired or distorted sound pronunciation.
Experts note that recently a new type of dyslalia has appeared - incorrect pronunciation of sounds T - D. These anterior lingual sounds appear in ontogenesis at the age of 3 - 4 years.
When pronouncing these sounds, children make typical mistakes:
- Replacing the front-lingual sounds “T – D” with the corresponding back-lingual “K – G”, for example, “fuk(t)bolka”, “shk(t)ana”.
- Mixing the front-lingual consonants “T – D” with the back-lingual “K – G”: cell - cell; glass - rolled.
- The sound “T” can be softened by “P” or “K”, for example: pichka - bird; drink, drink instead of dot.
Reasons for incorrect sound pronunciation:
- Insufficient development of the articulatory apparatus.
- Violation of muscle tone of articulatory muscles.
- Underdevelopment of auditory perception (difficulty in differentiating sounds).
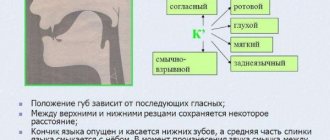
Articulatory structure of the T sound.
The sound T is front-lingual, consonant, hard, deaf. The sound D is anterior lingual, consonant, hard, voiced.
- The lips in a neutral position take the position of the next vowel sound,
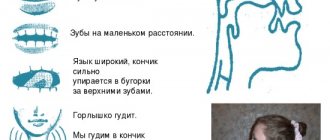
- The distance between the teeth is 5 mm.
- When pronouncing the vowel sounds A, O, U, Y, the tip of the tongue rests on the upper teeth or alveoli and forms a stop.
- The soft palate is raised, the vocal folds are open, the air stream is jerky
Features of sound production T - D
The classic techniques of speech therapy work are the preparatory stage and sound production.
1.Preparatory stage
Articulation gymnastics.
Speech therapy massage will help prepare the speech apparatus for it.
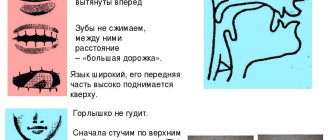
- “Wide smile” – connect your teeth, stretch your lips wide and hold this position for up to 7 seconds
- “Naughty Tongue” - say five-five-five, tapping your upper lip on your tongue, gradually differentiating (distinguishing) the sounds P-T.
- “Pancake” - relax the tongue, making it wide, and place it on the relaxed lower lip.
- “Rock” - raise the tongue only to the upper lip. We increase the rise of the tongue.
- “Grandfather’s mustache” - hold the cotton swab with your tongue on (above) your upper lip.
- “Sail” - a narrow tongue rests on the upper teeth - mast, raise the sail - a wide tongue. Alternation of narrow and wide language.
Exercise to form correct directed exhalation
- Blow out the candle - the child must purse his lips into a tube and sharply blow on the candle flame and extinguish it.
- Let's kick the ball into the goal. The child makes a gate out of bricks, places it in front of him, rolls a ball out of cotton wool and, smiling, blows hard on the ball, trying to get into the gate.
- “Snowflake” - the cotton wool is placed over the upper lip, the tongue covers the upper lip - inhale and exhale on the cotton wool.
The breathing exercise “Snowflake”, exercises for the tongue “Grandfather’s mustache”, “Rock”, “Sail” are quite effective in cases where the child has increased muscle tone of the tongue, and he cannot hold it near the teeth when exhaling.
2. Setting the sound T.
- Demonstration of correct lip and tongue position by showing
distinctions in pronunciation, for example, T (tip of the tongue) and K (tail of the tongue): “The cake is being eaten,” “Drops are dripping.”
- Imitation setting: an adult shows the position of the tongue and suggests repeating first the syllables and then the words.
- Interdental. The speech therapist asks the child to smile, bite the tip of his tongue with his teeth, and forcefully, sharply push the air forward. In this case, you can control the exhalation with your hand or blow on a cotton ball.
- Setting T from the sound P. The child repeats pa-pa-pa, placing the wide tip of the tongue on the lower lip, then, smiling broadly, pronounces P, which turns out to be T.
- Setting from Ts. I propose this technique from the opposite: the sound Ts “hides” two sounds behind itself - s-t.
“The cat catches the mouse” - we invite the child to imitate the movement of the cat’s claws with his fingers, straining his fingers and saying: tsap, tsap, tsap.
Then we shorten the syllable - tsa, tsa, tsa.
And here we are near the mink - we say Ts, Ts, Ts more and more quietly. Here you need to ask the child to only hit the teeth with the tongue - the T sound, do not pronounce the C sound.
- When setting D, the work is identical, only when exhaling the voice is added.
Automation of sounds T D
The sound is on. The beginning of a new stage: automation. All work on automation and differentiation of the studied sound consists of developing the skills of recognition and correct pronunciation of sound in syllables, words and sentences. It is important to achieve free pronunciation, while not forgetting about articulatory gymnastics.
The correct selection of articulatory and breathing exercises, exercises, and verbal material will help to obtain good results in the development of competent, beautiful speech in a child.
This is a long, labor-intensive process that requires patience and hard training. With systematic and regular work on the sounds T and D, it is possible to achieve positive results, i.e. create sounds, automate them and introduce them into the child’s speech.
Causes of dysarthria
Most often (in 65-85% of cases) dysarthria accompanies cerebral palsy and has the same causes. In this case, organic damage to the central nervous system occurs in the prenatal, birth or early periods of child development (usually up to 2 years). The most common perinatal factors of dysarthria are toxicosis of pregnancy, fetal hypoxia, Rhesus conflict, chronic somatic diseases of the mother, pathological course of labor, birth injuries, at birth, kernicterus of newborns, prematurity, etc. The severity of dysarthria is closely related to the severity of motor disorders in cerebral palsy : Thus, with double hemiplegia, dysarthria or anarthria is detected in almost all children.
In early childhood, damage to the central nervous system and dysarthria in a child can develop after suffering neuroinfections (meningitis, encephalitis), purulent otitis media, hydrocephalus, traumatic brain injury, severe intoxication.
The occurrence of dysarthria in adults is usually associated with a stroke, head injury, neurosurgery, and brain tumors. Dysarthria can also occur in patients with multiple sclerosis, amyotrophic lateral sclerosis, syringobulbia, Parkinson's disease, myotonia, myasthenia, cerebral atherosclerosis, neurosyphilis, oligophrenia.
Diagnosis of dysarthria
The examination and subsequent management of patients with dysarthria is carried out by a neurologist (children's neurologist) and speech therapist. The extent of the neurological examination depends on the expected clinical diagnosis. The most important diagnostic value is given by electrophysiological studies (electroencephalography, electromyography, electroneurography), transcranial magnetic stimulation, MRI of the brain, etc.
Speech therapy examination for dysarthria includes assessment of speech and non-speech disorders. Assessment of non-speech symptoms involves studying the structure of the articulatory apparatus, the volume of articulatory movements, the state of facial and speech muscles, and the nature of breathing. The speech therapist pays special attention to the history of speech development. As part of the diagnosis of oral speech in dysarthria, a study of the pronunciation aspect of speech (sound pronunciation, tempo, rhythm, prosody, speech intelligibility) is carried out; synchronicity of articulation, breathing and voice production; phonemic perception, level of development of the lexico-grammatical structure of speech. In the process of diagnosing written speech, tasks are given for copying text and writing from dictation, reading passages and comprehending what is read.
Based on the examination results, it is necessary to distinguish between dysarthria and motor alalia, motor aphasia, and dyslalia.
Symptoms of dysarthria
The speech of patients with dysarthria is slurred, unclear, and incomprehensible (“porridge in the mouth”), which is due to insufficient innervation of the muscles of the lips, tongue, soft palate, vocal folds, larynx, and respiratory muscles. Therefore, with dysarthria, a whole complex of speech and non-speech disorders develops, which constitute the essence of the defect.
Impaired articulatory motor skills in patients with dysarthria may manifest as spasticity, hypotonia, or dystonia of the articulatory muscles. Muscle spasticity is accompanied by constant increased tone and tension in the muscles of the lips, tongue, face, and neck; tightly closed lips, limiting articulatory movements. With muscle hypotonia, the tongue is flaccid and lies motionless on the floor of the mouth; the lips do not close, the mouth is half open, hypersalivation (salivation) is pronounced; Due to paresis of the soft palate, a nasal tone of voice appears (nasalization). In the case of dysarthria occurring with muscular dystonia, when attempting to speak, muscle tone changes from low to increased.
Sound pronunciation disturbances in dysarthria can be expressed to varying degrees, depending on the location and severity of damage to the nervous system. With erased dysarthria, individual phonetic defects (sound distortions) and “blurred” speech are observed.” With more pronounced degrees of dysarthria, there are distortions, omissions, and substitutions of sounds; speech becomes slow, inexpressive, slurred. General speech activity is noticeably reduced. In the most severe cases, with complete paralysis of the speech motor muscles, motor speech becomes impossible.
Specific features of impaired sound pronunciation in dysarthria are the persistence of defects and the difficulty of overcoming them, as well as the need for a longer period of automation of sounds. With dysarthria, the articulation of almost all speech sounds, including vowels, is impaired. Dysarthria is characterized by interdental and lateral pronunciation of hissing and whistling sounds; voicing defects, palatalization (softening) of hard consonants.
Due to insufficient innervation of the speech muscles during dysarthria, speech breathing is disrupted: exhalation is shortened, breathing at the time of speech becomes rapid and intermittent. Voice disturbances in dysarthria are characterized by insufficient strength (quiet, weak, fading voice), changes in timbre (deafness, nasalization), and melodic-intonation disorders (monotony, absence or inexpressibility of voice modulations).
Due to slurred speech in children with dysarthria, auditory differentiation of sounds and phonemic analysis and synthesis suffer secondarily. The difficulty and insufficiency of verbal communication can lead to an undeveloped vocabulary and grammatical structure of speech. Therefore, children with dysarthria may experience phonetic-phonemic (FFN) or general speech underdevelopment (GSD) and associated corresponding types of dysgraphia.
Causes of errors in pronunciation
- The sounds themselves are pronounced differently from ours (different articulation gives a different sound).
- These sounds are not softened before front vowels , as in Russian (yes, they do not have a pair of soft sounds. At all!).
- At the end of a word, these sounds are not deafened (reduction of voiced consonants is one of the most common mistakes).
Another article on the topic: How can I speak English if my language is Russian?
Today we will work on each point according to a scheme familiar to our readers: first theory, and then practice on special sets of words and tongue twisters.
Paired sounds in English: exercises
Again, I will repeat a typical mistake for us - deafening the final sound and thus changing the meaning of the word: bu zz
- bu s (buzz - bus), ri se - ri ce (rise - rice)
. Listen to how Stephen Curtis Chapman pronounces the /z/ sound in the song “His Eyes.”
Hi s
eye
s
are alway
s
upon us;
Hi s
eye
s
never clos
e
in sleep.
And no matter where you go, You will alway s
be in Hi
s
eye
s
, in Hi
s
eye
s
.
(His eyes are always looking at us, his eyes never close in sleep. And no matter where you go, you will always be in his eyes)
From 0:47 to 1:11
Task No. 5.
You know it