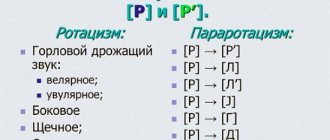
Rhoticism is considered to be a speech defect when the pronunciation of [r] is difficult or not possible at all.
The sound can be produced in different ways, just not correctly. This is hissing, whistling, etc.
Today we will talk about this speech defect. There is another very similar defect - pararotacism, which occurs when the pronunciation of [рь] is impaired.
Pararotacism is sometimes distinguished as a type of rhotacism, since the distortion concerns the same sound [p], only in its soft form.
For example, instead of “crow” you can hear various variations of the word “voyona”, “volona” or “vogona”, but not the right one.
But we will learn more about pararotacism in one of the following articles.
Rotacism in speech therapy
In speech therapy, rhotacism is usually called distortion or absence of the sound [p] in speech.
Previously, this phenomenon was called burring.
With this deficiency, a person (usually a child) tries to growl, but vibration does not occur.
Instead of “fish” one hears “yba”, “handle” - “uchka”, etc.
If you ask what exactly is the difference between rhotacism and pararotacism, then it will be enough to remember that with rhotacism the sound is distorted or absent, and with pararotacism [r] is replaced with a sound that is easier for a particular child. Most often it is L.
Rotacism occurs in children, both without diagnoses of speech development, and with dyslalia, rhinolalia or dysarthria.
In general, the sound [r] is considered the most difficult to articulate. It requires a lot of tension on the muscles and the tip of the tongue.
More than 26% of preschoolers suffer from such a speech defect. And children with erased dysarthria have 50% of rhoticism in addition to other symptoms of the disorder.
Features of sigmatism
- The defect in speech is built symmetrically, that is, if a hard sound suffers, then the soft one is also distorted.
- If only soft sibilants are used, then the sibilants will be pronounced softer.
- Nasal sigmatism is also determined, but it does not exist as such. If there is a nasal pronunciation of whistling and hissing sounds, then the pronunciation of all sounds will be nasal, and this is rhinolalia. However, nasal sigmatism can occur in deaf and mute people when sounds are presented to them.
- Hissing and whistling sounds are sharply contrasted in terms of acoustic characteristics, but less contrasting in terms of articulation.
Phonetic characteristics of sound [P]
[R] is a consonant sound. Since both noise and voice are involved in its pronunciation, it is sonorant.
Formed in the front of the tongue, trembling.
Since the air comes out through the mouth, this is the sound of the mouth.
Correct articulation of a single P will only occur if:
- open your lips;
- teeth in an open position;
- the tongue rises like a cup and overlaps the alveoli (this place is located immediately behind the upper teeth);
- the air is exhaled with a slight pressure directly onto the tip of the tongue and vibration is obtained.
During the process of phonation, the soft palate is raised and the passage to the nasal cavity is closed.
The folds close, begin to vibrate slightly, and a ringing R is obtained.
When pronouncing soft P, the tip of the tongue approaches the incisor teeth, and the back of the tongue begins to rest against the palate.
In this case, R is pronounced briefly and with one beat.
Types and forms of rotacism
In domestic speech therapy you can find studies by various authors in terms of the classification of rhotacism.
Some offer as many as 30 types of pronunciation defects [P]. Others settle on several forms.
We will focus on eight varieties as the most common.
Uvular rotacism
In the larynx of each of us there is a small tongue-like process called the uvular process.
When the sound [R] is pronounced using this process, the sound is very close to normal R.
This is exactly how the Germans pronounce R. It also somewhat resembles the French R. I think it’s very beautiful. Although in scientific speech therapy circles it is considered a violation.
But this is in domestic speech therapy, since such a pronunciation does not suit Russian R.
Velar rhotacism
With velar rotacism, although the soft palate vibrates, instead of P, only a rough rumble is obtained.
Like uvular, velar rhotacism is usually called gular rhotacism. Among the people, it’s just burr.
Lateral rotacism
If the vibration occurs along the edges of the tongue, then the result is RL. It is easy to hear and identify the form of burr.
Buccal rotacism
When pronouncing P, the air stream can pass between the edges of the tongue and the cheeks. The result is a slight vibration of either one or both cheeks.
In this case, a little noise is added to the voice.
Single-beat rotacism
In this case, the tongue is in the correct position, but vibration does not occur.
Instead of P you get English D.
Bilabial rhoticism
With this method of sound pronunciation, there is vibration of the lips, although the tongue does not move.
Instead of P, PRR is heard.
Nasal rotacism
The air stream can pass through the nose. Then NG is heard, since the tongue is motionless.
Glottal rhoticism
The laryngeal form of sound pronunciation resembles the velar one. However, the sound is somewhat muffled. It looks more like a slotted G.
For clarity, we show the forms of rotacism with their signs and causes of occurrence in the table.
Speech therapy. Proficiency test with answers (2021) - option 63
content .. 61 62 63 64 ..Question No. 1
What is the unit of the syntactic code of a language? 1) word; 2) morpheme; 3) offer. (+)
Question No. 2
Which structural and functional block will you predict is unformed when you identify errors in substitutions of paired consonants in written work: 1) block of regulation of tone and wakefulness; 2) block for receiving information processing and storage; (+)
3) programming, regulation and control unit.
Question No. 3
The soft palate vibrates with the following type of rhotacism: 1) single-beat; 2) velar; (+)
3) uvular;
4) there is no correct answer. Question No. 4
Carrying out work on differentiating sounds in pronunciation is not necessary for: 1) pararotacisms; 2) rotacisms; (+)
3) pararotacisms;
4) parasigmatisms. Question No. 5
Disadvantages in the pronunciation of voiced consonants, expressed in the replacement of voiced consonants with paired voiceless sounds, are called a) voicing defects (+)
b) defects in softening c) defects in the pronunciation of palatal sounds
Question No. 6
Working on speech with motor alalia involves (exclude unnecessary things) 1) normalization of breathing and voice formation; (+)
2) impact on the entire speech system;
3) the use of sign-symbolic activity; 4) use of subject-based practical activities. Question No. 7
The etiological factors causing stuttering include: 1) the state of the central nervous system; 2) the presence of mental trauma; 3) genetic factor; 4) all answers are correct;
(+)
Question No. 8
Clinical and pedagogical classification of speech disorders is based on: 1) on a set of psychological and linguistic criteria; 2) on a set of psychological, linguistic and clinical criteria; (+)
3) on psychological criteria;
4) on linguistic criteria. Question No. 9
Continue the statement: “FFNR is...” 1) violation of the pronunciation side of speech; (+)
2) unformed lexical and grammatical categories;
3) violation of the syllabic structure of the word. Question No. 10
For which of the listed types of speech disorders is “silent mode” used as the first stage of speech therapy work? 1) rhinophonia 2) alalia 3) bradyllalia 4) tachylalia (+)
Question No. 11
What principle of Russian spelling requires the writing of words in accordance with the rules: 1) phonetic; 2) morphological; (+)
3) traditional.
Question No. 12
What is the unit of the phonological code of a language: 1) word; 2) phoneme; (+)
3) morpheme.
Question No. 13
Which voice register should be practiced in people who stutter at the initial stages of work on developing the skills of rational voice delivery: 1) head; 2) chest; (+)
3) average.
Question No. 14
What is the unit of the lexical code of a language: 1) word; (+)
2) phoneme;
3) offer. Question No. 15
Violation of the processes of formation of the pronunciation system of the native language in children with various speech disorders due to defects in the perception and pronunciation of phonemes is. a) general speech underdevelopment b) phonetic-phonemic speech underdevelopment (+) c) aphasia
Question No. 16
Which term characterizes congenital shortening of the frenulum of the tongue: 1) microglossia; 2) glossoptosis; 3) progeny; 4) ankyloglossia.
(+)
Question No. 17
Speech disorders are characterized by the following features: (exclude the wrong answer) a) They correspond to the age of the speaker (+)
b) Associated with deviations in the functioning of the psychophysiological mechanisms of speech c) Often have a negative impact on the further mental development of the child d) They are stable and do not disappear on their own
Question No. 18
What sound attack is used when working on voice delivery with people who stutter: 1) firm, 2) aspirated, (+)
3) soft.
Question No. 19
If the structure of the organs of the articulatory apparatus is disturbed, a violation of sound pronunciation most often manifests itself in the form of 1) omission 2) replacement 3) confusion 4) distortion
(+)
Question No. 20
The subject of speech therapy as a science is: a) speech disorders and the process of training and education of persons with speech disorders (+)
b) a person (an individual suffering from a speech disorder; c) a pathological mechanism that determines the occurrence and development of speech disorders.
Question No. 21
Which of the listed cranial nerves does not innervate the organs of the peripheral speech apparatus? 1) trigeminal; 2) olfactory; (+)
3) wandering.
Question No. 22
What is the name of the phenomenon when a sound is pronounced as unusual in the phonetic system of the native language in terms of its acoustic effect (abnormal reproduction of sounds due to incorrectly formed individual articulatory positions? a) distortion (+) b) confusion c) interchange
Question No. 23
The leading mechanism for the speech development of students and pupils is (choose the correct option, answer one): 1. individual approach; 2. formation of neoplasms; (+)
3. intact intelligence and intact innervation of the peripheral speech apparatus;
4. the ability to express thoughts through speech and writing Question No. 24
Passive repetition of individual words or phrases without understanding their meaning is called: 1) logorrhea; 2) paraphasia; 3) hyperacusis; 4) echolalia. (+)
Question No. 25
The correct spelling of which sentence requires the assimilation and implementation of the phonetic principle of Russian spelling: 1) Here is my house. 2) Here is my parachute. 3) Here is my dog.
(+)
Question No. 26
The semantic level of speech activity is: (choose the correct answer) 1) the ability to formulate speech in acts of articulate articulation (syntagmas) (+)
2) the ability to use familiar words 3) the ability to distinguish speech signals by ear 4) the ability to write a dictation without errors
Question No. 27
On the basis of what documents is the speech therapy center of a general education institution completed (exclude the wrong answer 1): 1. PMPK extracts and statements from parents; 2. conclusions of the speech therapist and statements from parents; 3. conclusions of an otolaryngologist and statements from parents; 4. existing standards for the coverage of speech therapy correction for students and statements from parents
(+)
Question No. 28
This type of dysarthria occurs when the subcortical nuclei are damaged 1) extrapyramidal (+)
2) pseudobulbar 3) bulbar 4) cortical
Question No. 29
Restorative training is. a) a two-way controlled process, including the active cognitive activity of children in acquiring knowledge, skills and abilities and pedagogical guidance of this activity b) a process in which correction and compensation of the personal characteristics of persons with speech impairments are carried out (+)
c) a process that is aimed at restoring impaired speech and non-speech functions
Question No. 30
What method is used to teach literacy to preschoolers with speech disorders: 1) the sound method; 2) sound-syllabic method; 3) sound analytical-synthetic method; (+)
4) it is not recommended to teach preschoolers with speech disorders to read and write.
Question No. 31
R. E. Levina classified replacements and mixtures of sounds as. (what) defects in which the language system is disrupted a) phonological b) phonemic (+) c) anthropophonic
Question No. 32
What is not included in the main tasks of the preparatory stage for the formation of correct sound pronunciation a) development of auditory attention, auditory memory and phonemic perception b) elimination of insufficient development of speech motor skills, conducting preparatory speech exercises for the development of mobility of the organs of the peripheral speech apparatus c) elimination of incorrect sound pronunciation
(+)
Question No. 33
A speech therapist teacher needs to select a specific task for a six-year-old child in order to study the state of phonemic analysis and synthesis. Which of the tasks corresponds to the goal? 1) task with highlighting a given sound from words (against the background of words) 2) task with highlighting the stressed vowel at the beginning of a word 3) task with highlighting the first consonant in a word 4) task with determining the sequence of sounds in a word
(+)
Question No. 34
If a child pronounces “pulka” instead of the word “bun”, this may indicate that he has: 1) a defect in voicing; (+)
2) softening defect;
3) stunning defect; 4) there is no correct answer. Question No. 35
A form of dysarthria in which voluntary motor skills of the articulatory apparatus are impaired (in terms of manifestation in the sphere of sound pronunciation it resembles motor alalia) a) bulbar b) cortical (+)
c) cerebellar
Question No. 36
The defect in the pronunciation of the sounds [р] and [рь] is called. a) pararotacism b) rhotacism (+)
c) sigmatism
Question No. 37
Mark which of the listed symptoms of stuttering does not relate to psychopathological symptoms: 1) convulsions; 2) obsessive states; 3) asthenic syndrome.
(+)
Question No. 38
In accordance with the order of the Ministry of Education and Science dated December 24, 2010. No. 2075 “On the duration of working hours (standard hours of teaching work for the wage rate) of teaching staff” - the weekly workload of a speech therapist teacher in educational institutions is: (choose the correct answer) 1) a speech therapist teacher has an irregular work week 2) 20 hours per week week (+)
3) 24 hours a week 4) 36 hours a week
Question No. 39
Which speech disorder does not belong to the communication disorders identified within the psychological and pedagogical classification? 1) OHP, 2) stuttering, (+) 3) FFN,
Question No. 40
What violations of sound pronunciation are an indicator of alalia in the differential diagnosis of it with dysarthria: 1) distortion; (+)
2) omissions;
3) replacements. Question No. 41
What is not one of the causes of functional dyslalia? a) pedagogical neglect b) underdevelopment of phonemic hearing c) shortened frenulum of the tongue
(+)
Question No. 42
Speech-auditory memory is impaired in the following type of aphasia: 1) afferent-motor; 2) acoustic-mnestic; (+)
3) acoustic-gnostic;
4) the same for all types of aphasia. Question No. 43
What is the unit of the morphological code of a language: 1) word; 2) morpheme; (+)
3) offer.
Question No. 44
This speech disorder is caused by anatomical and physiological defects of the speech apparatus: 1) dyslalia; 2) rhinolalia; (+)
3) stuttering;
4) alalia. Question No. 45
Clinical and pedagogical classification of speech disorders includes (exclude the wrong answer): 1. violation of the means of communication 2. violation of the phonation (external) design of the statement 3. violation of the structural-semantic design of the statement 4. violation of written speech
(+)
Question No. 46
What disorder causes paralysis or paresis of the speech muscles: 1) dyslalia; 2) dysarthria; (+)
3) stuttering.
Question No. 47
Which speech disorder primarily affects the fluency and rhythm of speech: 1) alalia; 2) stuttering; (+)
3) dyslalia.
Question No. 48
Select the main biological factor in the occurrence of alalia: 1) organic damage to the speech zones of the left hemisphere; 2) left hemisphere organic damage to the central nervous system; 3) bilateral organic damage to the central nervous system.
(+)
Question No. 49
What speech disorder is caused by organic damage to the peripheral part of the speech motor analyzer? 1) alalia, 2) mechanical dyslalia (+)
3) aphasia,
Question No. 50
Which of the following areas is the most important in the initial stages of working with non-speaking children with motor disabilities according to the language approach: a) enrichment and activation of subject vocabulary; (+)
b) formation and development of articulatory motor skills;
c) development of auditory perception; d) enrichment and activation of the predicative vocabulary. Question No. 51
Phonemic perception is: 1) mental actions to analyze or synthesize the sound structure of a word; 2) special mental actions to differentiate phonemes and establish the sound structure of a word; (+)
3) subtle, systematized hearing, which has the ability to carry out operations of discrimination and recognition of phonemes that make up the sound shell of a word;
4) there is no correct answer. Question No. 52
What is the primary defect in optical dysgraphia, dyslexia: 1) impaired phonemic hearing: 2) impaired phonetic hearing; 3) violation of the generalized optical image of the letter
(+)
Question No. 53
With the help of what control is the feedback mechanism carried out in the speech functional system? 1) tactile, 2) visual, 3) kinesthetic
(+)
Question No. 54
If the structure of the organs of the articulatory apparatus is disturbed, disturbances in sound pronunciation most often manifest themselves in the form of: 1) confusion; 2) replacement; 3) distortions; (+)
4) passes;
Question No. 55
What is the unit of the lexical code of a language: - word (+)
Question No. 56
What is meant by exogenous-organic causes of speech disorders? 1) incorrect speech of others; 2) bilingualism in the family; 3) traumatic brain injury.
(+)
Question No. 57
Practical methods of speech therapy include: 1) games, exercises, modeling; (+)
2) observation, looking at drawings;
3) story, conversation, reading; 4) all answers are correct. Question No. 58
Which of the researchers proposed to establish the levels of development of active speech (zero, situational, nominative, predicative, dissected)? 1) R.E. Levin 2) N.S. Zhukova (+)
3) G.V. Chirkina 4) T.B. Filicheva
Question No. 59
In what disorder does increasing sound volume in most cases not improve auditory perception, and sometimes even worsens it (exhaustion of auditory function occurs)? 1) hearing loss; 2) sensory alalia; (+)
3) motor alalia;
4) aphasia. Question No. 60
One of the characteristics of general underdevelopment of speech of the third level (GSD-III level) according to R.E. Levina is (choose the correct answer option 1): 1. active vocabulary in a “rudimentary” state, consists mainly of sound pronunciations and babbling words ; 2. relatively detailed speech, the active vocabulary is dominated by nouns and verbs; (+)
3. enrichment of speech through the use of certain forms of inflection;
4. passive dictionary, no active understanding of speech Question No. 61
Determine the sequence of types of work to develop phonemic analysis: A. Determine the number of sounds in a word; B. Determine whether a given sound is in a word; B. Come up with a word with 4 sounds; D. Determine the place of the sound in the word (beginning, middle, end). 1) GBAV; 2) BGAV; 3) BAGV.
(+)
Question No. 62
On what sounds do stutterers most often experience cramps during speaking: 1) stop consonants; 2) vowels; (+)
3) fricative consonants.
Question No. 63
Bradylalia is. a) pathologically slow speech rate (+)
b) pathologically accelerated rate of speech c) a violation of the dark-rhythmic organization of speech caused by a convulsive state of the muscles of the speech apparatus
Question No. 64
A change in the shade of voice timbre caused by a violation of the relationship of the nasal cavity with the oropharyngeal resonator in the process of phonation is 1) aphonia 2) rhinophonia (+ )
3) dysphonia 4) phonasthenia
Question No. 65
Continue the definition of “ONR is ...”: 1) violation of the pronunciation aspect of speech; 2) systemic underdevelopment of all components of the language system; (+)
3) violation of pronunciation due to insufficient innervation of the articulatory apparatus.
Question No. 66
Child S. has a written speech disorder. Which of the mistakes made by the child when completing written assignments from the teacher indicate the presence of dysgraphia based on a violation of the processes of language analysis - synthesis? 1) replacement of letters 2) underwriting of elements (+)
3) omission of letters and syllables 4) spelling errors
Question No. 67
Violation of sound pronunciation with normal hearing and intact innervation of the speech apparatus is ... a) rhinolalia b) alalia c) dyslalia (+)
Question No. 68
What type of dyslexia is caused by underdevelopment of the grammatical structure of speech, morphological and syntactic generalizations? 1) agrammatic dyslexia (+)
2) mnestic dyslexia 3) optical dyslexia 4) semantic dyslexia
Question No. 69
What is the unit of the syntactic code of a language? -suggestion (+)
Question No. 70
What is the outdated name for dyslalia? a) nasality b) muteness c) tongue-tied
(+)
Question No. 71
The structure of a speech defect is understood as: a) a set of signs (manifestations) of a speech disorder b) a set (composition) of speech and non-speech symptoms of a given speech disorder and the nature of their connections (+)
c) the nature of deviations in the functioning of processes and operations that determine the occurrence and development of speech disorders.
Question No. 72
Who was one of the first in Europe to introduce the term “dyslalia” into scientific circulation? a) V. Oltushevsky b) R. Schulthess c) I. Frank (+)
Question No. 73
Choose the correct sequence of tasks for the development of spatial orientation: A. Determining the position of objects in relation to the right-left hand; B. Determination of spatial relationships between three objects; C. Orientation in one’s own body; D. Determination of spatial relationships between 2 objects. 1) SADB; (+)
2) ASBD;
3) DBAS. Question No. 74
What is the name of the course of speech pathology in which there is an increase in symptoms of speech pathology: 1) regressive; 2) remitting; 3) stationary; 4) progressive.
(+)
Question No. 75
What is the leading form of activity in preschool age? a) objective-action b) game (+)
c) emotionally positive communication with an adult
Question No. 76
Who first formulated the principles of analysis of speech disorders? a) R. E. Levin (+)
b) F. F. Pay c) M. E. Khvattsev
Question No. 77
What does the child’s transition from physiological tongue-tiedness to dyslalia based on the type of distortions in the pronunciation of speech sounds indicate: 1) a lag in the formation of phonemic hearing; 2) about progress in the formation of phonemic hearing; (+)
3) about the primary inferiority of the organs of articulation.
Question No. 78
The main areas of activity of a speech therapist teacher do not include: (choose the correct answer) 1) primary diagnosis of a child’s speech development 2) psychological correction of personality traits (+)
3) advisory activities 4) speech therapy correction
Question No. 79
Which of the following tasks cannot be used to assess understanding of the meaning of what was read: 1) detailed retelling, 2) answers to questions about what was read; 3) a brief retelling, 4) drawing up a plan for the text read.
(+)
Question No. 80
What form of stuttering is caused by psychogenic causes (psychotrauma): 1) neurosis-like; (+)
2) organic;
3) neurotic. Question No. 81
The pedagogical process aimed at correcting and compensating for speech impairments, at raising and developing a child with a speech impairment is. a) correction of speech disorders b) speech therapy (+)
c) compensation
Question No. 82
Which variant of incorrect writing of a sentence indicates that the child’s phonemic concepts are not formed: 1) There was a vase of roses on the table. (+)
2) There was a vasa with dew on the table.
3) On etol etoyala vaea e roeami. Question No. 83
What type of prevention is aimed at preventing the chronicity of stuttering: 1) primary; (+)
2) secondary;
3) tertiary. Question No. 84
At what stage of the formation of reading skills identified by T.G. Egorov, there is a semantic guess at the level of the entire text: 1) the level of syllable-analytical reading; 2) the stage of development of synthetic reading techniques; 3) stage of synthetic reading.
(+)
Question No. 85
What may underlie a violation of the organization of the tempo-rhythmic aspect of speech: 1) organic damage to the extrapyramidal system; 2) organic damage to the medulla oblongata 3) organic damage to the cerebellum.
(+)
Question No. 86
Which of the following speech disorders refers to disorders of the internal formulation of utterances? 1) bradyllia 2) aphasia (+)
3) dyslalia 4) dysphonia
Question No. 87
What causes articulatory-acoustic dysgraphia? 1) violation of various forms of language analysis and synthesis 2) underdevelopment of the grammatical structure of speech 3) underdevelopment of visual gnosis, analysis and synthesis, spatial representations 4) reflection of incorrect pronunciation in writing
(+)
Question No. 88
What principle of examining children with alalia aims to study all aspects of speech, as well as non-verbal mental functions: 1) an integrated approach; (+)
2) systematic approach;
3) ontogenetic. Question No. 89
A four-year-old child is in a lesson with a speech therapist. What word should the teacher choose to reproduce the sound-syllable structure for the child? 1) cabbage (+)
2) tomatoes 3) frying pan 4) medicine
Question No. 90
Identify specific errors characteristic of phonemic dyslexia: 1) substitution of graphically similar letters; 2 violation of the sound-syllable structure of the word; (+)
3) changing the form and tense of verbs.
Question No. 91
If instead of the word “tomato” a child pronounces “bamidor”, then this may indicate that he has 1) a softening defect 2) a voicing defect 3) a deafening defect (+)
4) there is no correct answer
Question No. 92
Indicate what is an important prerequisite for successful literacy learning: 1) the idea of sound; 2) the idea of a grapheme; 3) idea of the phoneme.
(+)
Question No. 93
The features of the speech activity of students with moderate and severe mental retardation are (one correct answer): 1. lack of planned speech in preschool age, poor vocabulary, sentences in oral speech are often constructed incorrectly and are not complete ; written language contains many specific errors; 2. speech with a poorly developed regulatory function, absence of adjectives and adverbs in speech, in most situations “the child’s speech is idling” (M.S. Pevzner); (+)
3. delayed mastery of the grammatical structure of speech, pronunciation defects, limited active vocabulary, difficulties in mastering written language;
4. pathologically slow speech rate and reading rate, inability to briefly retell the text, come up with a title for a story Question No. 94
Erased forms of pseudobulbar dysarthria are often confused with 1) alalia 2) dyslalia (+) 3) rhinolalia 4) all answers are correct
Question No. 95
What is the unit of the phonological code of a language: -phoneme (+)
Question No. 96
Erroneous reproduction of words, which consists in combining syllables belonging to different words into one word, is called: 1) perseveration; 2) anticipation; 3) contamination; (+)
4) accommodation.
Question No. 97
Disorders of the structural and semantic design of statements include: 1) alalia; (+)
2) rhinolalia;
3) dyslalia; 4) all answers are correct. Question No. 98
What rate of speech is typical for stuttering: 1) intermittent; (+)
2) accelerated;
3) slow Question No. 99
What term refers to persistent, repeated errors associated with difficulties in mastering and applying spelling rules: a) calligraphic; b) spelling; c) dysorthographic.
(+)
Question No. 100
What is the cause of motor and oculomotor dysgraphia and dyslexia: 1) impaired phonemic hearing; 2) phonetic hearing impairment; 3) violation of hand, finger praxis or oculomotor functions
. (+)
content .. 61 62 63 64 ..
Types of rotacism Table
| Form | Signs | Causes |
| Complete absence of sound | The sounds [р], [рь] are omitted completely in speech, replaced by vowels | There is no articulatory movement of the tongue and lips necessary for sonorous sounds |
| Velar rhotacism | The vibration is erratic; instead of a growl, a noise mixed with a voice is heard. During phonation, the back and root of the uvula are moved toward the posterior palate, forming a closure between the organs and the upper palate. The air passes between them in jerks, so noise is generated, there is almost no voice | Short hypoglossal ligament |
| Uvular rotacism | The tip of the tongue does not vibrate enough and interferes with the passage of the air stream. There is a growl, but there is little noise in it | Short hypoglossal ligament |
| Lateral rotacism | There is vibration, but it is unclear due to the shift in the place of its origin. The tip of the tongue or its sides close with the lateral parts of the palate, or during articulation the back of the tongue rises. As a result, the sound softens or slips | Paresis, high and narrow palate, short hypoglossal ligament, developmental defect of the upper jaw |
| Nasal rotacism | Phonation occurs through the nose, it is not pronounced [r], but the German ng | Short soft palate (congenital defect), incomplete velopharyngeal seal |
| Bilabial rhoticism | Only the lips vibrate, the tongue remains motionless | Paresis, weak muscles of the speech apparatus |
| One-hit | Full vibration is replaced by a weak rumble. Articulation gives English d. When spoken, the tongue contacts the alveoli not with a series of vibrating blows, but once. | Paresis, other articulatory disorders |
| Buccal rotacism | The air stream does not pass along the body of the tongue and the upper palate, but from the side, the cheeks vibrate | Incorrect placement of organs during articulation: the tongue is lowered, the tip is not pressed to the palate |
Yotacism
Replacing the letter "y" with "l". There are three defects in the pronunciation of back-lingual sounds:
- Gamacism - sound "g"
- Kappacism - the sound "k"
- Hitism (x) - replacing the sounds “x” with “f”, especially before “v”. Or "хх" on "х". For example, cunning - cunning.
Gamacism and cappacism are usually found together in practice. They are characterized by:
- The absence of the sounds “G” and “K”.
- Replacing “k” and “g” with “t” and “d”. For example, a rabbit is a troll.
- Replacing "k" with "k".
All these defects arise due to certain systems of activity. Most sounds are front-lingual and these sounds are also pronounced as front-lingual.
Reasons for rotacism
Rhotacism itself is a disorder resulting from such speech disorders as: mechanical dyslalia, dysarthria, open rhinolalia.
Children with FFND and OHP are often susceptible to rotacism.
Factors in the development of rotacism are considered:
- Anomaly of the tongue. This may be a short frenulum that prevents the tongue from moving up.
- Anomaly of the dental system. Cleft palates and side bites allow air to leak through the gap. Likewise, the hard palate is a complication for the articulation of R.
- Weak articulatory muscles. They interfere with the correct pronunciation of the sounds R and Rb. There is practically no vibration of the tongue, so the stream of exhaled air is too weak.
- Problems with phonemic hearing. The child simply does not match the correct sound with the one he himself pronounces. but this is rare. Most often, the sound is simply replaced with one that is easier for the child to pronounce.
- Dysarthria. Here uvular and velar rhotacism takes place. Frequent cases are lateral distortion, which leads to pareticity of the cheeks and tongue.
- Bilingualism and imitation. If the family also speaks another language (uvular - if in French, or guttural - if German is heard in the family), then the child simply imitates the pronunciation without even noticing.
Features of complex dyslalia
The more complex the combination of dyslalia, the more complex the background against which it occurs: a delay in general and mental development. In cases of complex dyslalia, an in-depth additional study of the child is necessary, not only in terms of the characteristics of his behavior, but also intellectual capabilities, as well as characteristics of hearing and vision. Complex dyslalia is a signal that something is wrong with the child’s hearing or vision. In children with hearing impairments, very often the front-lingual sounds are either sharply distorted or replaced by the sound “t”.
If a child has hearing loss of the 2nd or 3rd degree, then an auxiliary criterion will be the peculiarity of the voice; it lacks the necessary metal, the voice seems to be “cotton-like.”
Children with severely reduced vision and blind children may also experience pronunciation defects such as complex dyslalia. This is due to the fact that in such children, sigmatism occurs 3-4 times more often than in the norm. This is due to visual control. But if we establish a connection between interdental sigmatism and visual defects, then, consequently, all hearing-impaired people should have interdental sigmatism, but this is not the case. After all, the child does not see the sounds “k”, “g”, “n” - they are not impaired, but they have complex dyslalia.
A visual defect interferes with speech in general - the blind do not speak by imitation, the visually impaired cannot ask anything, they are passive. Initiative speech develops by age 4. The pronunciation system is formed when the teeth begin to change, hence interdental sigmatism appears. Complex dyslalia occurs against the background of delayed speech communication due to visual defects.
With hearing defects, disorders of the maxillomuscular system are often encountered: progenia, prognathism, anterior open bite, lateral open bite.
Diagnostics
As a rule, a speech therapist can diagnose rhotacism. He talks with the child’s parents to rule out the fact of bilingualism in the family.
After this they carry out:
- Examination of articulation organs. Examine the structure of the lips, a number of teeth, tongue, soft and hard palate. It is important to examine the oral cavity for the presence of a short frenulum or malocclusion. You should also find out if there is a facial cleft, etc. It is also necessary to determine whether any form of dystonia is progressing.
- Study of the mobility of the articulatory apparatus. The specialist examines the tongue and lips, gives several test tasks to determine volume, tempo, accuracy, switchability of movements and the ability to hold an articulatory pose.
- Analysis of phonemic hearing. A specialist tests speech hearing using exercises to differentiate isolated sounds at the level of words and syllables.
- Sound pronunciation examination. Using special exercises, a speech therapist studies how correctly a child pronounces isolated sounds in different parts of a word. At the same time, a conclusion is made about the type of rotacism. It is very important to prescribe the correct correction program.
Pararotacism
Pararotacism in speech therapy is the replacement of rumbling [p] and soft [рь] with phonemes that are simpler for the speaker. The cause of difficulty in articulation will be paresis, a shortened hyoid frenulum, impaired phonemic hearing, and imitation of adults. May be a form of dyslalia.
Among the types of pararotacism, the following replacements of the sound [r] can be distinguished:
- [v]: pronounced without vibration: ruka-wuka
- [d]: fish-fish
- [g]: steam-pag
- [l]: mole-klot, [l] is more often pronounced in the soft version - [l]
- [s]: chamomile - ymashka
- [th]: mouth – yot.
If we talk about factors predisposing to rhotacism and pararotacism, pediatricians, neurologists and speech therapists identify the following congenital and acquired causes:
- Birth injuries
- Bilingualism in the family
- Heredity
- Anatomical anomalies in the development of the articulatory apparatus
- Hearing impairment
- Malocclusion
- Injuries of the tongue, jaw
Methods for correcting rotacism
There are various speech therapy tools for correcting speech disorders due to rhoticism.
Sometimes it is simply impossible to cope with this illness using such means.
Therefore, you have to resort to medical help. For example, to correct a short frenulum defect, it will need to be trimmed.
If there is an incorrect bite, then you will need to wear braces for some (sometimes long) time.
Also, some medications help achieve the desired effect.
But this appointment should be made, for example, by a neurologist.
The basis of correctional work for rotacism is special classes with a speech therapist.
As a rule, work is carried out in stages: the preparatory stage, production and automation of sounds, transition and strengthening of speech.
Preparatory stage
First, it is necessary to acquaint a person with the correct articulation of the sounds [P] and [P'].
Visual aids help in this case - drawings, diagrams, presentations.
Sound video slides have proven themselves very well, when the student not only hears the sound, but also sees how the tongue is positioned and the lips stretch.
Sound files can be played multiple times.
Previously, a speech therapist did all this - he pronounced it, showed it to himself.
Now technology has come to the rescue. On the computer, everything can be clearly seen and heard.
Repeated playback of the recording makes the specialist’s task easier.
At the preparatory stage, they show what the exhalation should be like when pronouncing the sounds [P] and [P'].
Carrying out articulatory gymnastics contributes to:
- development of lifting the tongue upward;
- activate the tip of the tongue;
- learn to vibrate your tongue;
- stretch the hypoglossal ligament.
Next comes breathing work. Exercises are selected by a speech therapist.
He also provides speech therapy to the masses if the need arises.
Articulation and breathing exercises must be performed not only in the speech therapist’s office, but also at home.
Doing these exercises at home at least twice a day will prepare you for the main lessons on producing and automating the sounds [P] and [P'].
It should be noted that the preparatory stage is very important.
And until the skills to maintain an articulatory posture and control exhalation are formed, you should not move on to the next stage.
The student must have a strong directed air stream.
Preparatory phase exercises
Preparing the speech organs for the articulation of R-R, which is sonorous, will help master vibration.
The following exercises will prepare the speech apparatus, help stretch the hyoid ligament and help develop the elasticity of the tongue.
Exercise "Horse"
The tongue is pressed against the upper palate followed by a clicking sound.
The volume and tempo of the clicks can be changed.
Exercise "Coachman"
Thanks to this exercise, the labial muscles develop.
During the execution, you need to close your mouth, make your lips vibrate and at this time pronounce in a drawn-out manner “whoa-oo-oo-oo-oo-oo”, and then “tr-r-r-r-r”.
Exercise "Painter"
This exercise is necessary in order to stretch the frenulum under the tongue.
To do this, the tongue is pulled up, then with the tip we begin to stroke the upper palate.
Exercise “Toothbrush”
When smiling, you need to stick out the tip of your tongue and brush your teeth. The tongue should move along the outer surface of the teeth, and then along the inner.
The movements are slow, the jaws are in a fixed position.
Exercise "Swing"
The tongue in a spread-out state should be raised, placed behind the upper row of teeth, and then lowered behind the lower teeth.
The mouth opens only a few centimeters.
Exercise "Drummer"
This exercise will help train the tip of your tongue.
The mouth does not open wide, the tongue is placed behind the lower teeth, while it is necessary to knock and pronounce “d-d-d-d.”
The pace increases slowly and gradually.
This set of exercises is carried out not only during the preparatory stage.
They are also used to warm up the muscles at the beginning of each speech therapy session, when correction of rotacism is planned.
In terms of time, these workouts initially last for 15-20 minutes, and subsequently the duration increases to 30 minutes.
Staging stage
Different forms of rotacism require different approaches to corrective measures.
But as practice shows, differentiated methods of sound production work most effectively.
It is possible to achieve a pronunciation that would correspond to the norm of the Russian language:
- in an imitative way - for example, imitate the growl of a dog or lion, the caw of a crow or the sounds of a car engine;
- proceed from the reference sounds D and Zh;
- multiple “td”, “j”;
- articulation exercises;
- mechanical assistance for correcting vibration of the tip of the tongue using a positioning probe or its substitute.
In rare cases, sound production is carried out in two stages (for example, with buccal rotacism).
At the initial stage, they work on the proto sound, and then vibration is worked on.
The development of soft R follows the delivery of hard R, followed by access to iotized or I.
There is a universal method that is used by speech therapists to eliminate rotacism.
Includes several steps:
- Setting up the fricative R from Zh. The child is taught to pronounce the sound without stretching the lips, the tongue rises to the alveoli. In this position, growling is required. The sound is dull, the air stream is strong. With this sound, sound is introduced into open syllables.
- The production of full vibration begins using a ball probe. The umbrella is passed along the bottom of the tongue back and forth while pronouncing the fricative phoneme. Movements must be fast. The air stream is strong and pressure. At home, you can use a teaspoon instead of a probe. This method is most effective when working with sonorants.
Another method is called mixed. It is used only in rare cases when the ball probe did not help produce the correct sound.
With a mixed method:
- The performance begins with the syllable ZA - the child pronounces the syllable many times, while the tongue smoothly moves upward to the alveoli. The result should be a fricative R.
- When P is combined with A, massage begins with an elongated probe and the tip of the tongue is raised to the palate. The probe moves from left to right and gradually P becomes clear and not drawn out.
- It is possible to build on other vowels. For example, from iotized ones: U, O, E, Y.
- To get Py, they push off from ZI. The diagram is the same as in the exercise just above.
Automation
Automation of the correct pronunciation of the sound Р-Рь is carried out in a playful way, starting from very simple, easy exercises with gradual complication.
Speech material is selected in the following sequence:
- syllables, rows of syllables (forward, reverse);
- words with a given sound found in different parts of the word;
- phrases;
- offers;
- pure talk.
Next, poems and stories with a large number of P/Pb are taken.
The duration of correctional classes for rotacism ranges from one and a half to three months.
In rare cases it may be more. Individual characteristics, causes of the defect, regularity of exercises, as well as the skill of the speech therapist - all this affects the duration of sound pronunciation correction.
The most difficult thing is to come to the correct pronunciation of P/Pb with dysarthria. With this diagnosis, speech therapy assistance may be required for months or even years.
Corrective work with children is usually carried out in a playful way. Small and interesting poems and visual material are used.
First, the speech therapist achieves good vibration, the hard version of P, and only then moves on to automating the soft one.
In syllables
You can't come up with any creativity when working with syllables. This is normal repetition. Multiple.
But it is possible to diversify tasks.
First, these will be syllables beginning with the sound R. Then a group of syllables with the position P in the middle of the syllable. And the final stage is P at the end of the syllable.
Simple repetition quickly becomes boring.
Therefore, you can come up with little rhymes.
Ra-ra-ra - it's hot outside. Ro-ro-ro – there’s a bucket in the middle of the yard. Ru-ru-ru - I carry the bucket across the yard.
Tra-tra-tra - I go out into the yard in the morning. Three-three-three - how beautiful, look.
Ar-ar-ar - take a lantern with you.
Dre-dre-dre - crucian carp live in a bucket.
In words
- At first, it is better to take monosyllabic words, similar to three-letter syllables: world, gift, ball, shooting range, kar, boron, thief...
- Next, we use words consisting of two syllables, one of which contains R: mosquito, painter, fire...
- Next, we move on to reading words with P in the middle of the word: bucket, square, bloomers, peas, pie, cheers, mountain...
In phrases
The phrases should be funny so that the child is interested in working with them.
You can also make rhymes out of them.
Mischievous sparrow, don’t hit the mosquito.
It's time to bake a pie, don't forget about the cottage cheese.
We reinforce correct articulation in a playful way:
- The picture shows animals, among them... - a huge Lynx (the child finishes).
- A large, very large... - ruddy turnip grew in the garden bed.
- Put aside pictures with objects whose names contain the sound R and come up with phrases so that each word has an R (red pen, a beautiful primer, a huge lantern...).
Prevention of rotacism with a short hypoglossal ligament
The hyoid frenulum looks like a thin membrane that connects the sublingual area of the mouth with the tongue. With a normal structure, it is attached to the middle of the inner surface of the tongue, its length is about 8 mm.
To check the length of the child's frenulum, you need to ask him to touch the roof of his mouth with his tongue with his mouth wide open: a problem-free manipulation indicates a normal frenulum length. If, while performing the action, the child was unable to reach the sky or experiences discomfort, it is imperative to consult a speech therapist. If the frenulum is located too close to the tip of the tongue, it needs correction. It is performed to avoid speech problems, including the occurrence of rhoticism.
If the frenulum was not cut in infancy, it is trimmed during the preschool period. Pruning for preschoolers is done under local anesthesia. The frenulum is cut and self-absorbing sutures are applied. The latest technologies allow this operation to be performed using a laser. The laser method minimizes pain, reduces swelling after surgery, and eliminates the need for stitches. Postoperative rehabilitation includes a special diet and exercises to develop the frenulum.
An alternative way to correct a shortened hyoid ligament is articulation gymnastics. This is no less effective, and at the same time painless method. The essence is to perform speech therapy exercises for the language.
They usually tire the child very much and often provoke discomfort. Because of this drawback, they should be performed under the supervision of a speech therapist, gradually increasing the load. Non-surgical stretching of a shortened frenulum requires a long period of time.